US ECONOMICS
CORONAVIRUS
The White House. May 19, 2020. President Trump’s letter to the WHO
The World Health Organization’s response to Coronavirus has been filled with one misstep and cover-up after another. American taxpayers send over $400 million to the WHO each year—about 10 times what China gives—for the privilege of watching this UN agency parrot Chinese government claims and put political correctness over saving lives.
President Trump halted this funding last month until the WHO’s mismanagement of the pandemic is investigated. In the meantime, the United States is redirecting global health aid to other groups directly engaged in the fight.
This week, President Trump sent a letter to Dr. Tedros, Director-General of the WHO, outlining 14 serious concerns raised by America’s review of the agency. Here’s an excerpt:
The World Health Organization has repeatedly made claims about the coronavirus that were either grossly inaccurate or misleading . . . You praised the Chinese government for its "transparency" with respect to the coronavirus, announcing that China had set a "new standard for outbreak control" and "bought the world time." You did not mention that China had, by then, silenced or punished several doctors for speaking out about the virus and restricted Chinese institutions from publishing information about it.
THE WHITE HOUSE. EXECUTIVE ORDERS. May 19, 2020. ECONOMY and JOBS. Executive Order on Regulatory Relief to Support Economic Recovery
In December 2019, a novel coronavirus known as SARS-CoV-2 (“the virus”) was first detected in Wuhan, Hubei Province, People’s Republic of China, causing an outbreak of the disease COVID-19, which has now spread globally. The Secretary of Health and Human Services declared a public health emergency on January 31, 2020, under section 319 of the Public Health Service Act (42 U.S.C. 247d), in response to COVID-19. In Proclamation 9994 of March 13, 2020 (Declaring a National Emergency Concerning the Novel Coronavirus Disease (COVID-19) Outbreak), I declared that the COVID-19 outbreak in the United States constituted a national emergency, beginning March 1, 2020.
I have taken sweeping action to control the spread of the virus in the United States, including by suspending entry of certain foreign nationals who present a risk of transmitting the virus; implementing policies to accelerate acquisition of personal protective equipment and bring new diagnostic capabilities to laboratories; and pressing forward rapidly in the search for effective treatments and vaccines. Our States, tribes, territories, local communities, health authorities, hospitals, doctors and nurses, manufacturers, and critical infrastructure workers have all performed heroic service on the front lines battling COVID-19. Executive departments and agencies (agencies), under my leadership, have helped them by taking hundreds of administrative actions since March, many of which provided flexibility regarding burdensome requirements that stood in the way of implementing the most effective strategies to stop the virus’s spread.
The virus has attacked our Nation’s economy as well as its health. Many businesses and non-profits have been forced to close or lay off workers, and in the last 8 weeks, the Nation has seen more than 36 million new unemployment insurance claims. I have worked with the Congress to provide vital relief to small businesses to keep workers employed and to bring assistance to those who have lost their jobs. On April 16, 2020, I announced Guidelines for Opening Up America Again, a framework for safely re-opening the country and putting millions of Americans back to work.
Just as we continue to battle COVID-19 itself, so too must we now join together to overcome the effects the virus has had on our economy. Success will require the efforts not only of the Federal Government, but also of every State, tribe, territory, and locality; of businesses, non-profits, and houses of worship; and of the American people. To aid those efforts, agencies must continue to remove barriers to the greatest engine of economic prosperity the world has ever known: the innovation, initiative, and drive of the American people.
By the authority vested in me as President by the Constitution and the laws of the United States of America, it is hereby ordered as follows:
Section 1. Policy. It is the policy of the United States to combat the economic consequences of COVID-19 with the same vigor and resourcefulness with which the fight against COVID-19 itself has been waged. Agencies should address this economic emergency by rescinding, modifying, waiving, or providing exemptions from regulations and other requirements that may inhibit economic recovery, consistent with applicable law and with protection of the public health and safety, with national and homeland security, and with budgetary priorities and operational feasibility. They should also give businesses, especially small businesses, the confidence they need to re-open by providing guidance on what the law requires; by recognizing the efforts of businesses to comply with often-complex regulations in complicated and swiftly changing circumstances; and by committing to fairness in administrative enforcement and adjudication.
Sec. 2. Definitions.
(a) “Emergency authorities” means any statutory or regulatory authorities or exceptions that authorize action in an emergency, in exigent circumstances, for good cause, or in similar situations.
(b) “Agency” has the meaning given in section 3502 of title 44, United States Code.
(c) “Administrative enforcement” includes investigations, assertions of statutory or regulatory violations, and adjudications by adjudicators as defined herein.
(d) “Adjudicator” means an agency official who makes a determination that has legal consequence, as defined in section 2(d) of Executive Order 13892 of October 9, 2019 (Promoting the Rule of Law Through Transparency and Fairness in Civil Administrative Enforcement and Adjudication), for a person, except that it does not mean the head of an agency, a member of a multi-member board that heads an agency, or a Presidential appointee.
(e) “Pre-enforcement ruling” has the meaning given it in section 2(f) of Executive Order 13892.
(f) “Regulatory standard” includes any requirement imposed on the public by a Federal regulation, as defined in section 2(g) of Executive Order 13892, or any recommendation, best practice, standard, or other, similar provision of a Federal guidance document as defined in section 2(c) of Executive Order 13892.
(g) “Unfair surprise” has the meaning given it in section 2(e) of Executive Order 13892.
Sec. 3. Federal Response. The heads of all agencies are directed to use, to the fullest extent possible and consistent with applicable law, any emergency authorities that I have previously invoked in response to the COVID-19 outbreak or that are otherwise available to them to support the economic response to the COVID-19 outbreak. The heads of all agencies are also encouraged to promote economic recovery through non-regulatory actions.
Sec. 4. Rescission and waiver of regulatory standards. The heads of all agencies shall identify regulatory standards that may inhibit economic recovery and shall consider taking appropriate action, consistent with applicable law, including by issuing proposed rules as necessary, to temporarily or permanently rescind, modify, waive, or exempt persons or entities from those requirements, and to consider exercising appropriate temporary enforcement discretion or appropriate temporary extensions of time as provided for in enforceable agreements with respect to those requirements, for the purpose of promoting job creation and economic growth, insofar as doing so is consistent with the law and with the policy considerations identified in section 1 of this order.
Sec. 5. Compliance assistance for regulated entities.
(a) The heads of all agencies, excluding the Department of Justice, shall accelerate procedures by which a regulated person or entity may receive a pre-enforcement ruling under Executive Order 13892 with respect to whether proposed conduct in response to the COVID-19 outbreak, including any response to legislative or executive economic stimulus actions, is consistent with statutes and regulations administered by the agency, insofar as doing so is consistent with the law and with the policy considerations identified in section 1 of this order.
Pre‑enforcement rulings under this subsection may be issued without regard to the requirements of section 6(a) of Executive Order 13892.
(b) The heads of all agencies shall consider whether to formulate, and make public, policies of enforcement discretion that, as permitted by law and as appropriate in the context of particular statutory and regulatory programs and the policy considerations identified in section 1 of this order, decline enforcement against persons and entities that have attempted in reasonable good faith to comply with applicable statutory and regulatory standards, including those persons and entities acting in conformity with a pre-enforcement ruling.
(c) As a result of the ongoing COVID-19 pandemic, the Department of Health and Human Services, including through the Centers for Disease Control and Prevention, and other agencies have issued, or plan to issue in the future, guidance on action suggested to stem the transmission and spread of that disease. In formulating any policies of enforcement discretion undersubsection (b) of this section, an agency head should consider a situation in which a person or entity makes a reasonable attempt to comply with such guidance, which the person or entity reasonably deems applicable to its circumstances, to be a rationale for declining enforcement under subsection (b) of this section. Non-adherence to guidance shall not by itself form the basis for an enforcement action by a Federal agency.
Sec. 6. Fairness in Administrative Enforcement and Adjudication. The heads of all agencies shall consider the principles of fairness in administrative enforcement and adjudication listed below, and revise their procedures and practices in light of them, consistent with applicable law and as they deem appropriate in the context of particular statutory and regulatory programs and the policy considerations identified in section 1 of this order.
(a) The Government should bear the burden of proving an alleged violation of law; the subject of enforcement should not bear the burden of proving compliance.
(b) Administrative enforcement should be prompt and fair.
(c) Administrative adjudicators should be independent of enforcement staff.
(d) Consistent with any executive branch confidentiality interests, the Government should provide favorable relevant evidence in possession of the agency to the subject of an administrative enforcement action.
(e) All rules of evidence and procedure should be public, clear, and effective.
(f) Penalties should be proportionate, transparent, and imposed in adherence to consistent standards and only as authorized by law.
(g) Administrative enforcement should be free of improper Government coercion.
(h) Liability should be imposed only for violations of statutes or duly issued regulations, after notice and an opportunity to respond.
(i) Administrative enforcement should be free of unfair surprise.
(j) Agencies must be accountable for their administrative enforcement decisions.
Sec. 7. Review of Regulatory Response. The heads of all agencies shall review any regulatory standards they have temporarily rescinded, suspended, modified, or waived during the public health emergency, any such actions they take pursuant to section 4 of this order, and other regulatory flexibilities they have implemented in response to COVID-19, whether before or after issuance of this order, and determine which, if any, would promote economic recovery if made permanent, insofar as doing so is consistent with the policy considerations identified in section 1 of this order, and report the results of such review to the Director of the Office of Management and Budget, the Assistant to the President for Domestic Policy, and the Assistant to the President for Economic Policy.
Sec. 8. Implementation. The Director of the Office of Management and Budget, in consultation with the Assistant to the President for Domestic Policy and the Assistant to the President for Economic Policy, shall monitor compliance with this order and may also issue memoranda providing guidance for implementing this order, including by setting deadlines for the reviews and reports required under section 7 of this order.
Sec. 9. General Provisions.
(a) Nothing in this order shall be construed to impair or otherwise affect:
(i) the authority granted by law to an executive department or agency, or the head thereof; or
(ii) the functions of the Director of the Office of Management and Budget relating to budgetary, administrative, or legislative proposals.
(b) This order shall be implemented consistent with applicable law and subject to the availability of appropriations.
(c) Notwithstanding any other provision in this order, nothing in this order shall apply to any action that pertains to foreign or military affairs, or to a national security or homeland security function of the United States (other than procurement actions and actions involving the import or export of non-defense articles and services).
(d) This order is not intended to, and does not, create any right or benefit, substantive or procedural, enforceable at law or in equity by any party against the United States, its departments, agencies, or entities, its officers, employees, or agents, or any other person.
THE WHITE HOUSE. May 18, 2020. REMARKS. ECONOMY & JOBS. Remarks by President Trump in a Meeting on Opportunity Zones
THE PRESIDENT: Okay. Thank you very much. We’re here talking about Opportunity Zones and other things having to do with economic development and also the inner cities. And Tim Scott — Senator Tim Scott of South Carolina has been with us on Opportunity Zones from day one. He first approached me and he mentioned it, and I loved the idea. And who knew it was going to be so successful, Tim. Right?
SENATOR SCOTT: Tremendous.
THE PRESIDENT: So it’s —
SENATOR SCOTT: Thank you for your support.
THE PRESIDENT: Well, thank you for your support and for your knowledge.
And if I might, I’d like to have Tim start off by saying a few words, and then Scott Turner, executive director, has done an incredible job. And, Scott, we’d like to hear from you too, okay?
Tim, please.
SENATOR SCOTT: Well, thank you, sir. Mr. President, thank you for your commitment to all Americans. And truth be told, your commitment has gone beyond the voting booth. You’re helping people because they’re Americans, and you don’t care whether they’re Democrats or Republicans, whether they’re black or white, whether they’re up or they’re down, whether they’re rich or they’re poor. Your focus is making sure that America is healthier as we come out of this COVID-19. And I thank you personally for your support of all people, but specifically to the underserved community.
And what we have before us today, sir, is a way for us to improve the economic outcomes, to improve the health outcomes, and in the long view of what we think is in the best interest of connecting people to the opportunities that will change their lives. And from an economic development perspective, I always think about capital and competency. The more access to capital you have, the more competent you will be long term.
And the way that we have put structure together, it really provides people with more access to capital. The PPP has been a classic example of improving and expanding access to capital in such a way that businesses continue to succeed. Health outcomes — there are a myriad of ways of talking about it. I like to think about it from a testing and telemedicine — testing in the most vulnerable communities.
I think the emphasis has been on the nursing homes — we’ve learned a lot about that — and then those communities that have two or more health conditions — underlying health conditions. We see the highest hospitalization with our senior population as well as those folks with two or more comorbidities.
And so as we focus on testing and telemedicine, we’re creating access in the rural parts of our country in a way that we have not before. And you have led with real force on that topic, and I truly appreciate that.
And on the last one — the long-term structural change — I look at it from a connectivity perspective and choice perspective. So the connectivity — broadband — being incredibly important. I’ve heard you talk about that a thousand times, if I’ve heard you talk about it once. And then from a choice perspective, whether it’s charter schools or school choice, we have an opportunity to continue to change lives, and you’ve led on all those fronts. And I think we’re going to see tremendous impact.
And certainly, my baby, of course, is opportunity zones.
THE PRESIDENT: Right.
SENATOR SCOTT: You have been front and center. And I’m sure Scott is going to talk a lot about Opportunity Zones. But you have assembled the kind of firepower that our nation needs at a critical time. It’s one of the reasons why we’re going to have a V-shape as we hit August, September, October, November, in this economic recovery.
THE PRESIDENT: Well, I think so. And you’re seeing it maybe today for the first time, where not only are the markets up tremendously, but we’ve had tremendous — tremendously good and positive information on therapeutics, on cures, and on vaccines —
SENATOR SCOTT: Yes, sir.
THE PRESIDENT: — from some of the most respected companies in the world, and researchers and doctors and labs. And that’s coming in, and I think you’re very close to having a very, very positive situation. And, you know, with it understood — and we always talk about it, Tim — when you lost one person to this, it’s too many — just too many. And we’re talking about thousands and millions of people throughout the world, on something that should have never happened.
SENATOR SCOTT: Absolutely.
THE PRESIDENT: It should’ve been stopped in China. It should’ve been stopped at the source. But it happened.
But they’re coming out with tremendous — it’s incredible what they can do. And I’ve seen results, and the results are staggeringly good. So, I’m very happy.
And the market is up very big, and I think you’re going to have a “V.” I think it’s going to be terrific. I think we’re going to have a transition in the third quarter, Ben, and the transition is going to lead to a very good fourth quarter. And I think we’re going to have a year next year — because of all the stimulus and everything else, and the pent-up demand — like you haven’t seen in a long time.
SENATOR SCOTT: Oh, my gosh, 2021 is going to be amazing.
THE PRESIDENT: And the stock market is not very short of where it was with all that we went through. It’s — and that means a lot of smart people are looking and they’re saying, “We’re coming back. And we’re coming back to that level.” I think we’re going to come back to greater than that level.
And we’ve learned a lot. One of the things we’ve learned is being reliant on ourselves. Don’t be reliant on other countries that, frankly, maybe have different agendas. And frankly, there are plenty of them out there, so it’s one of those things.
So this is a very big day. This feels much different than Friday. Friday is a different feeling than today. This is a very positive day.
Ben Carson, would you like to say a few words?
SECRETARY CARSON: Well, first of all, thank you for redirecting us. You know, it was three weeks ago when you said the White House Opportunity and Revitalization Council should refocus — not get rid of, but add to its plate focusing on those individuals who are disadvantaged and who have suffered the most.
And I think this epidemic that we’re going through right now focused the light on the fact that there were some people who had significant disparities that put them at increased risk for the disease.
So you asked us to really get to the bottom of that. And it’s not just the fact that people have hypertension and diabetes and obesity and asthma. It’s the things that create an atmosphere where those things flourish.
THE PRESIDENT: Right.
SECRETARY CARSON: And so we’ve been really concentrating on getting at the underlying causes. And I think, first of all, you know, between myself and Ja’Ron, Jared, and a few others, we’ve talked to hundreds of thousands of stakeholders across the country in various communities to find out from them what their perspective was, particularly in terms of the CARES Act and how it was impacting them and what could be done differently.
And we have discovered some things which we are in the process of correcting. Some of it will require legislative help, and, you know, Senator Scott is all over that. So I think that’s going to get done. And the staff in all the agencies — you have 17 different agencies and councils who have been very much involved. Secretary DeVos have been very involved, particularly with the education, the broadband.
THE PRESIDENT: Good.
SECRETARY CARSON: The fact that this whole pandemic has changed a lot of things. But we are looking for positive ways to take advantage of that. For instance, with education, now it’s going to be possible to take the best biology teacher and put them in front of a million students instead of 30 students. So a lot of those people who were not getting a good education, if we do this the right way, we can provide an excellent education for them.
THE PRESIDENT: That’s right.
SECRETARY CARSON: Same thing for workforces. So we’re looking at ways that we can take advantage of all these things. And this has been done very rapidly. Three weeks ago, you asked us to do this. And I just want to thank all the people who’ve been involved, all of the primaries and the various agencies. Everybody has been incredibly responsive. And this is going to get done.
THE PRESIDENT: Good. Thank you, Ben. Good job too. Thank you very much.
Scott Turner, would you say a little bit about Opportunity Zones and how that’s all going?
MR. TURNER: Yes, thank you. And, Mr. President, I want to thank you for the opportunity to — really to not just be a part of the team, but to lead and to shepherd the White House Opportunity and Revitalization Council.
We were with you last in December when we had to do the one-year report, and now we are at a point to where we have a very strong foundation because of Opportunity Zones. And, as you know, we’ve traveled to over 60 cities across the country to convene stakeholders from the community — from businesses, education, faith leaders, elected officials — to convene at a table just like this to talk about, “Hey, what is the pain of the community? And what is the promise and the potential of the community?”
And those convenings have proven to bear a lot of fruit and given us, really, what we need from a partnership standpoint, from a coalition standpoint, and from a foundation standpoint now that we can go by your leadership and refocus, in the council, to go and implement these policies that we see here before us in our country. As you know, distressed communities generationally have been behind. And now, with the COVID and the recovery, you know, they have been severely hit. But we’re not discouraged from it, Mr. President. We are not discouraged, we’re not wavering, because we know that we have a strong team, we have great policies and — with your leadership and administration.
And Dr. Carson — Secretary Carson alluded to the agencies that are on the council. And everyone is passionate and compassionate about not just helping, but seeing our citizens across America in distressed communities thrive, from an entrepreneurship standpoint, from an economic standpoint, and really the spirit of this law.
And, Senator Scott, thank you for your leadership. Economic development and community social impact — and that’s what’s been going on across our country.
Yes, COVID is here, but our mission and the spirit is still the same, and now we’re just going to ramp it up.
THE PRESIDENT: Great.
MR. TURNER: You know, and keep going.
THE PRESIDENT: Thank you, Scott.
MR. TURNER: You’re welcome.
SECRETARY CARSON: And, Mr. President, this — this is —
(Secretary Carson presents a document.)
MR. TURNER: Yeah, that’s the best practices.
SECRETARY CARSON: Best practices. It shows you what’s going on in all the Opportunity Zones. It’s absolutely astonishing.
THE PRESIDENT: Very good.
SECRETARY CARSON: It’s very entertaining reading.
THE PRESIDENT: Very good.
SECRETARY CARSON: But you’d be amazed at what’s going on.
THE PRESIDENT: That’s good reading. Look at that. That’s good reading. (Laughter.) Let me just see something. Sixty-seven pages like that. (Laughter.) I don’t know. I’m not sure, Brooke, if I’m going to get to read all of it.
MS. ROLLINS: It looks —
THE PRESIDENT: But I’m going to try.
MS. ROLLINS: It looks — yeah, very stimulating.
THE PRESIDENT: I’m going to try.
MS. ROLLINS: For sure.
THE PRESIDENT: Brooke, you have a few words?
MS. ROLLINS: You know, I’ve —
THE PRESIDENT: Congratulations, by the way.
MS. ROLLINS: Oh, Mr. President, thank you so much. I think it’s really important to note that, just two and a half months ago, at the end of February, we were celebrating, I think, African American History Month. And we had over 800 African American leaders from around this country — of course, pre-COVID. And we — you stood up in front of that group of men and women and you talked about that. In just a few years, we had the lowest poverty rate in the history of our country for our African American population, our Hispanic population, our veteran population, our high school graduate population, our people with disabilities.
It was a remarkable time. And to be able to, sort of, celebrate that without knowing where we would be 10 weeks from that day, but now we know where we are. And looking back at what you were able to do with this country and lifting the forgotten Americans who are forgotten no more.
Now they’re in a tough spot again, but this is what this effort is entirely about — led by Dr. Carson, Senator Scott, and Scott Turner: How do we bring that prosperity not just back, but to even greater heights than it’s ever been before? I know you like to use the “transition to greatness,” and I think that’s 100 percent accurate in this case, and this is what this entire effort is about.
So thank you for convening this. Thank you for the redirection. And I know we’re all really excited.
THE PRESIDENT: We’ll bring it back.
MS. ROLLINS: Yes, we will.
THE PRESIDENT: We’ll bring it back.
MS. ROLLINS: Yes, we will.
THE PRESIDENT: Larry Kudlow, please.
MR. KUDLOW: Just to add to what the others have said, I think it’s a great project. I backed it wholeheartedly since the beginning. And Brooky mentions the low poverty rate we had before the virus struck and the low unemployment rate — and the low unemployment rate.
And one of the things I love about this initiative is we can spread prosperity and opportunity to every corner of the economy — every single corner of the economy: those who are underserved, those with poverty pockets. We can attract capital. We’re going to use private investment capital as the linchpin of this, and it will be rewarded in a number of different ways.
So, again, you rebuilt this economy. All right? We got hit by the virus. You’ll rebuild the economy again.
And you know what, sir? Besides the stock market, there are little glimmers. I don’t want to downplay the heartbreak because the numbers are not good for this quarter — bad, bad pandemic contraction — but there are little glimmers. A lot of the unemployed are temporary. We’re seeing evidence that gasoline demand is higher, that the Apple mobility charts are higher. That means more people are driving. We’ve seen the New York State Manufacturing Survey rise substantially. So there are little glimmers of hopes here and there.
THE PRESIDENT: A lot of things — a lot of things happening. Oil is —
MR. KUDLOW: Yes, sir.
THE PRESIDENT: — back up to a point where the energy industry is going to be — it may be in very good shape very soon.
MR. KUDLOW: Yeah.
THE PRESIDENT: So a lot of very important things are happening, and then the stock market sees it.
MR. KUDLOW: Yeah.
THE PRESIDENT: And that’s why the stock market is up so big. So it’s very good.
MR. KUDLOW: Thank you, sir.
THE PRESIDENT: Thank you all very much. Thank you.
U.S. Department of State. 05/19/2020. UPDATE: The United States Continues to Lead the Global Response to COVID-19
Through the American people’s generosity and the U.S. Government’s action, the United States continues to demonstrate global leadership in the face of the COVID-19 pandemic. The American people have given more than $10 billion that will benefit the global COVID-19 response, and we continue to ensure that the substantial U.S. funding and scientific efforts on this front remain a central and coordinated part of the worldwide effort against COVID-19. Months into fighting this pandemic at home and abroad, the United States continues to lead a global response—building on decades of leadership in life-saving health and humanitarian assistance.
Since the outbreak of COVID-19, the U.S. Government has committed more than $900 million in State Department and U.S. Agency for International Development (USAID) emergency health, humanitarian, economic, and development assistance specifically aimed at helping governments, international organizations, and non-governmental organizations (NGOs) fight the pandemic. This funding, provided by Congress, will save lives by improving public health education; protecting healthcare facilities; and increasing laboratory, disease-surveillance, and rapid-response capacity in more than 120 countries.
The United States has mobilized as a nation to make this an impressive global effort. Working with the private sector, we have begun to fulfill President Trump’s commitment to provide ventilators to our partners and allies in Africa, Asia, Europe, and Latin America. The first shipment of ventilators donated by the United States, through USAID, arrived in the Republic of South Africa on May 11, 2020. Our foreign assistance funding to date for the response to the COVID-19 pandemic includes an initial $23 million specifically to provide ventilators to some of these partners and allies. We expect to make future additional purchases and shipments of ventilators and related supplies.
The COVID-19 assistance to-date from the State Department and USAID includes the following:
- Nearly $300 million in emergency health assistance from USAID’s Global Health Emergency Reserve Fund for Contagious Infectious-Disease Outbreaks and Global Health Programs account. These funds prioritize interventions to mitigate the pandemic and prepare communities in developing countries affected and at-risk of COVID-19.
- Nearly $300 million in humanitarian assistance from USAID’s International Disaster Assistance (IDA) account. This assistance supports case management and keeps essential health services operating; provides risk communication and community engagement programs; supports infection, prevention, and control efforts; provides safe water and hygiene items; and strengthens local capacity and coordination by working with existing health structures and with others in the humanitarian community. These funds prioritize populations affected by ongoing humanitarian crises, particularly displaced people, because of their heightened vulnerability, the elevated risk of severe outbreaks in camps and informal settlements, and anticipated disproportionate mortality in these populations.
- More than $150 million from the Economic Support Fund (ESF) account. These funds promote American foreign-policy interests by financing shorter-term mitigation efforts and addressing the second-order impacts of the pandemic in the long term, across a variety of sectors.
- Nearly $160 million in humanitarian assistance from the Migration and Refugee Assistance (MRA) account, provided through the State Department’s Bureau of Population, Refugees, and Migration. These funds help international organizations and NGO partners address challenges posed by the pandemic in refugee, IDP, and host communities as well as other among migrants and other vulnerable people.
In addition to this direct funding from the U.S. Government, our All-of-America approach is helping people around the world through the generosity of American private businesses, non-profit groups, charitable organizations, faith-based organizations, and individuals, who have now provided more than $4.3 billion in donations and assistance globally, more than any other nation.
To meet the most urgent needs, U.S. Government Departments and Agencies are coordinating efforts to prioritize foreign assistance to maximize the potential for impact. The United States is providing the following assistance through the State Department and USAID:
Africa:
- Angola: $570,000 for health assistance is helping provide risk-communications and water and sanitation, and prevent and control infections in key health facilities in Angola. This assistance comes on top of long-term U.S. investments in Angola, which total $1.48 billion over the past 20 years, including over $613 million for health assistance.
- Bénin: $1.5 million in health assistance will help Béninois respond to the outbreak by funding the coordination and planning of outbreak-response activities, strengthening surveillance and rapid-response capabilities, and risk-communications and engagement with communities. This assistance joins $1.72 billion in total assistance for Benin over the past 20 years, over $364 million of which was for health.
- Botswana: $1.5 million in health assistance to address the outbreak. Funding will support risk-communications and community engagement, with a focus on the most vulnerable populations, the procurement of essential health commodities and logistic support, and strengthening case-management and the prevention and control of infections in key health facilities. This assistance builds on nearly $1.2 billion in total assistance in Botswana over the last 20 years, over $1.1 billion of which has been for health.
- Burkina Faso: Nearly $7 million in health and humanitarian funding will go toward risk-communications, water and sanitation, preventing and controlling infections in health facilities, public-health messaging, and more. This includes $2.5 million in health assistance, $1.5 million in IDA humanitarian assistance, and nearly $2.8 million in MRA humanitarian assistance, which will help protect the health of vulnerable people in Burkina Faso during the pandemic. Over the past 20 years, the United States has invested more than $2.4 billion total in Burkina Faso, including over $222 million for health alone.
- Burundi: More than $3 million in total funding for the response to COVID-19 includes $2 million in health assistance and more than $1 million in MRA humanitarian assistance to help protect the health of vulnerable people. The health assistance will improve the planning and coordination of response activities, the strengthening of surveillance and rapid-response capabilities, strengthening capacities for case-management and the prevention and control of infections, and the training of health workers. The United States has invested more than $997 million in total assistance for Burundi, including more than $254 million for health, over the past 20 years.
- Cameroon: Nearly $8 million for health and humanitarian assistance will help provide infection-control in key health facilities, strengthen laboratories and surveillance, prepare communities, and bolster local messaging. This includes $6.1 million for health and IDA humanitarian assistance from USAID, in addition to nearly $1.9 million in MRA humanitarian assistance to support refugees, IDPs, and host communities. This assistance builds upon more than $960 million in total U.S. investment in the country over the past 20 years, over $390 million of which has been for health.
- Central African Republic: More than $10 million in humanitarian assistance, including $6.5 million in IDA humanitarian assistance that will go toward risk-communications, preventing and controlling infections in health facilities, and safe water supplies, and more than $3.5 million in MRA humanitarian assistance that will help protect the health of vulnerable people in the Central African Republic during the pandemic. The U.S. Government has provided $822.6 million in total in the Central African Republic over the last 20 years, including $4.5 million in emergency health assistance in Fiscal Year (FY) 2019.
- Republic of Congo (ROC): $250,000 in health assistance will address the outbreak, by supporting the coordination and planning of response activities, risk- communications and community-outreach activities and the training of health workers in protocols for preventing and controlling infections in health facilities. The United States has invested in the Republic of Congo for decades, including more than $171.2 million in total U.S. assistance over the last 20 years, over $36.9 million of which has been for health.
- Chad: More than $3.5 million in humanitarian assistance, including $1 million from the IDA account for preventing and controlling infections in health facilities, raising community awareness of COVID-19, and improving hygiene, and nearly $2.6 million in MRA humanitarian assistance to help protect the health of vulnerable people in Chad during the pandemic. This new assistance builds upon the foundation of nearly $2 billion in total U.S. assistance over the last 20 years, including more than $30 million for health.
- Côte d’Ivoire: $3.2 million in health assistance to address the outbreak by financing risk-communications and community engagement; the training of health care providers in protocols for preventing and controlling infections in health facilities and the appropriate management of cases of COVID-19 and influenza-like illnesses; and ensuring these facilities are appropriately supplied with essential health commodities. Funding will also finance the training of health workers in critical community-level surveillance techniques, such as case-finding and contact-tracing. Over the past 20 years, the United States has invested more than $2.1 billion in long-term development and other assistance in Côte d’Ivoire.
- Democratic Republic of the Congo (DRC): More than $26 million in total including $16 million for health and IDA humanitarian assistance that will improve the prevention and control of infections in health facilities, and support improved awareness of COVID-19, including by working with religious leaders and journalists on risk-communication messaging. More than $5 million in MRA humanitarian assistance will help protect vulnerable people in the DRC during the pandemic. The $6 million of health assistance funding will support supply-chain management and logistics, as well as the procurement of essential health commodities; strengthening critical disease-surveillance activities, including community-based surveillance, contact-tracing, and case-finding; strengthening practices to prevent and control infections at health facilities and train health workers, as well as community-based efforts to improve access to water and basic hygiene materials, with the direct distribution of kits to households to prevent infections. Health assistance also will support mobilizing thousands of volunteers in targeted, high-risk Provinces to conduct risk-communications and community-engagement activities. Finally, approximately $5 million in ESF will go toward distance and alternative education for Congolese children and youth so they can continue to learn and maintain protective routines and social connections while schools remain closed across the country. This builds upon more than $6.3 billion in total U.S. assistance over the past 20 years, including more than $1.5 billion for health.
- Djibouti: $750,000 in total, including $500,000 in health assistance to address the outbreak and $250,000 in MRA humanitarian assistance to assist vulnerable migrants and host communities as they deal with the pandemic. Health assistance will support strengthening the capacity for testing, supply-planning, supply-chain management and the distribution of urgent health commodities needed for COVID-19. The health assistance also will fund risk-communications and community-outreach activities, the training of health workers to implement protocols to prevent and control infections in health facilities and manage cases of COVID-19; and disease-surveillance and rapid-response protocols and functionality. The United States has already invested more than $338 million in Djibouti over the last 20 years.
- Eswatini: $1.1 million in health assistance to address the outbreak by bolstering Eswatini’s emergency health response, which could include the procurement of supplies, contact-tracing, laboratory diagnostics, and raising public awareness. This assistance builds upon the foundation of U.S. Government investments in the Kingdom, which total more than $529 million assistance over the last 20 years, including more than $490 million for health.
- Ethiopia: More than $23.4 million in assistance to counter COVID-19, including $3.4 million for health and $7.5 million in IDA humanitarian assistance for risk-communications, the prevention and control of infections in health facilities, disease-surveillance, contact-tracing, and coordination; $7 million in ESF that will support continuing operation at a major industrial park in Hawassa to preserve critical jobs,; and more than $5.6 million in MRA humanitarian assistance for vulnerable people, including refugees, migrants, and host communities. The health assistance will support strengthening outbreak-response capabilities, including community-based surveillance for case-finding and contact-tracing; strengthening laboratory diagnostic capacity; and optimizing case-management and practices to prevent and control infections in health facilities. Health assistance will also fund risk-communications and community-engagement activities. This assistance is in addition to the United States’ long-term investments in Ethiopia over the past 20 years of more than $13 billion in total assistance, over $4 billion has been for health alone.
- Ghana: $1.6 million in health assistance to address the outbreak by strengthening outbreak-response capabilities, including community-based surveillance for case-finding and contact-tracing; improve laboratory diagnostic capacity; optimize the management of COVID-19 cases and the prevention and control of infections in health facilities; and promote risk-communications and community-engagement activities. This new assistance builds upon $3.8 billion in total U.S. Government investments in Ghana over the last 20 years, including over $914 million for health.
- Guinea: $1.3 million in health assistance to address the outbreak by financing risk-communications and community-outreach activities, the training of health workers to implement protocols to prevent and control infections in health facilities; and disease-surveillance and rapid-response protocols and functionality. The United States has invested nearly $1 billion in total assistance in Guinea over the last 20 years, including over $365.5 million for health.
- Kenya: Nearly $4.4 million for health and humanitarian assistance, including $3.5 million in health and IDA humanitarian assistance to bolster risk-communications; prepare health-communication networks and media for possible cases; and help provide public-health messaging for media, health workers, and communities; and $947,000 in MRA humanitarian assistance for refugees and host communities. This assistance specific to COVID-19 comes on top of long-term U.S. Government investments in Kenya, which total $11.7 billion over the last 20 years, including more than $6.7 billion for health alone.
- Lesotho: $750,000 in health assistance to address the outbreak by strengthening outbreak-response capabilities, including community-based surveillance for case-finding and contact tracing, strengthening laboratory diagnostic capacity, and optimizing case-management and the prevention and control of infections in health facilities. The health assistance also will finance risk-communications and community-engagement activities. This new assistance builds upon decades of U.S. investments in Lesotho, which total more than $1 billion over the last 20 years, including more than $834 million for health.
- Liberia: $1.3 million for health assistance will provide critical aid for all 15 Liberian Counties (emergency operation centers, training, contact-tracing, hospitals, and community health care), support quarantine efforts, and provide village-level support. The United States has helped lay a strong foundation for Liberia’s response to COVID-19 through more than $4 billion in total assistance over the past 20 years, including more than $675 million for health.
- Madagascar: $2.5 million in health assistance to address the outbreak by strengthening laboratory capacity for diagnostics; deploying mobile laboratories for decentralized diagnosis; improving regional and District surveillance, including data systems and the training of community health volunteers in contact-tracing; promoting risk-communications and community-engagement activities, including a staffed hotline, mass-media campaigns and prevention messages; the training of health professionals infection and prevention control training, procurement of essential health commodities, and improvements in waste management. The United States has invested more than $1.5 billion in total assistance for Madagascar over the last 20 years, including over $722 million for health alone.
- Malawi: $4.5 million in health assistance to address the outbreak. Funding will support the COVID-19 response and preparedness activities at the district level, including surveillance activities, strengthening infection and prevention control practices, screening at points of entry, and case management. Funding will also support risk communication and community engagement, including radio and social media campaigns; and technical assistance to optimize supply chain logistics and management. The United States has provided more than $3.6 billion in total assistance for Malawi over the past 20 years, including more than $1.7 billion for health.
- Mali: More than $8.4 million in assistance for the response to COVID-19, which includes $2.4 million for health assistance and $2 million in IDA humanitarian assistance for risk-communications, the prevention and control of infections in health facilities, and coordination; and more than $4 million in MRA humanitarian assistance to support vulnerable in Mali during the pandemic. Health assistance will support risk-communications and community engagement, including by establishing community communication networks with modern and traditional and to call on citizens to counter misinformation and rumors, as well as support to the Ministry of Health’s National Hotline; strengthening diagnostic networks and disease-surveillance systems, optimizing real-time surveillance to accelerate the detection and investigation of cases and contact-tracing and train and mobilize existing community-surveillance, early-warning and emergency rapid-response teams to report infections and assist ill persons in getting prompt and appropriate care. The health funding also will finance activities to prevent and control infections at priority case-detection points (including points of entry to Mali along high-traffic cargo routes) and public and community health facilities, including through the procurement of equipment and supplies to prevent infections and manage medical waste. This new assistance builds upon decades of U.S. investments in Mali, which total more than $3.2 billion over the last 20 years, including more than $807 million for health.
- Mauritania: $250,000 in health assistance to address the outbreak by financing risk-communications and community-engagement activities, strengthening supply-chain management and logistics, and improving the prevention and control of infections in health facilities. The United States has provided more than $424 million in total assistance over the last 20 years for Mauritania, including more than $27 million for health, which builds a strong foundation for their pandemic response.
- Mauritius: $500,000 in health assistance to address the outbreak under the national response strategy for COVID-19, including by strengthening coordination and logistics; developing and disseminating risk-communications and prevention materials at the community level; strengthening protocols for the prevention and control of infections in health facilities; disseminating case-management guidelines and training health workers in their use; improving surveillance and rapid-response protocols and functionality; and expanding laboratory capacity. This new assistance builds upon the foundation of more than $13 million in total U.S. Government investments over the past 20 years, including more than $838,000 for health.
- Mozambique: $6.8 million, including $4.8 million for health assistance and $2 million in IDA humanitarian funding will finance risk-communications and community engagement, including mass-media prevention messages; water and sanitation; and the prevention and control of infections in key health facilities in Mozambique. The health assistance also will fund the training of health workers in case-management and ensuring health facilities are prepared to respond to the outbreak. The United States has invested nearly $6 billion in Mozambique over the past 20 years, including more than $3.8 billion for health.
- Namibia: $750,000 in health assistance to address the outbreak by improving laboratory capacity for diagnostics and technical assistance in supply-chain management and logistics. This new assistance comes in addition to nearly $1.5 billion in total U.S. Government investments to Namibia over the past 20 years, including more than $970.5 million in long-term health assistance.
- Niger: Nearly $5.4 million in assistance includes nearly $800,000 million for health assistance and $2 million in IDA humanitarian assistance for risk-communications, the prevention and control of infectious diseases in health facilities, and coordination; and more than $2.6 million in MRA humanitarian assistance will support vulnerable people in Niger during the pandemic, including refugees, and vulnerable migrants, and host communities. This assistance comes on top of more than $2 billion in total U.S. Government investments for Niger in the past 20 years, nearly $233 million for health alone.
- Nigeria: More than $30.3 million in assistance, which includes more than $3.3 million for health assistance and $23 million in IDA humanitarian funding for risk-communications, water and sanitation, infection-prevention, and coordination; and nearly $4.1 million in MRA humanitarian assistance for vulnerable people. This assistance joins more than $8.1 billion in total assistance for Nigeria over the past 20 years, including more than $5.2 billion in U.S. health assistance.
- Rwanda: $2.2 million in assistance for Rwanda’s response to COVID-19 includes $1.7 million for health assistance that will help with disease-surveillance and case-management, and $474,000 in MRA humanitarian assistance to support refugees and host communities in Rwanda. This comes on top of long-term U.S. Government investments in Rwanda that total more than $2.6 billion in total assistance over the past 20 years, including more than $1.5 billion for health.
- Sénégal: $3.9 million in health assistance to support risk-communications, water and sanitation, the prevention and control of infections in health facilities, public health messaging, and more. In Sénégal, the U.S. has invested nearly $2.8 billion in total over the past 20 years, nearly $880 million for health.
- Sierra Leone: $1.7 million in health assistance to address the outbreak by strengthening surveillance activities, case-finding, contact-tracing, risk-communications, community engagement, and the management of cases of COVID-19 at health facilities. This assistance joins decades of U.S. investments in Sierra Leone, totaling more than $5.2 billion in total assistance over the past 20 years, including nearly $260 million for health.
- Somalia: More than $17.1 million, including $12.6 million in IDA and $4.5 million in MRA humanitarian assistance for the response to COVID-19 will fund risk-communications, the prevention and control of infectious diseases in health facilities, case-management, and more, including for refugee returnees, vulnerable migrants, and host communities. This assistance comes in addition to $5.3 billion in total assistance for Somalia over the last 20 years, including nearly $30 million for health.
- South Africa: Approximately $8.4 million in health assistance to counter COVID-19 will fund risk-communications, water and sanitation, the prevention and control of infections in health facilities, public health messaging, and more. The United States has also pledged to send up to 1,000 ventilators to South Africa, the first 50 of which arrived on May 11, 2020. This assistance joins more than $7 billion in total assistance by the United States for South Africa in the past 20 years, nearly $6 billion invested for health.
- South Sudan: Nearly $21.8 million in assistance for South Sudan’s response to COVID-19 includes $13.4 million in IDA humanitarian assistance for case-management, the prevention and control of infections, logistics, coordination efforts, risk-communications, water, sanitation and hygiene; $2.75 million in health programming; and more than $5.6 million in MRA humanitarian assistance that will support refugees, IDPs, and host communities in South Sudan during the pandemic. The health assistance will fund expanding the training of health workers and peer educators on proper practices to prevent and control infections in health facilities to protect communities and patients, particularly those at high risk or who are immunocompromised; strengthening capabilities in health facilities and in the community to manage and refer cases of COVID-19. The health assistance also will fund expanding efforts to address community concerns, including by tracking and combating rumors, misconceptions, and grievances. This funding builds upon past U.S. investments in South Sudan totaling $6.4 billion over the past 20 years, including more than $405 million for health.
- Sudan: More than $24.1 million in assistance includes $16.8 million in IDA humanitarian assistance for strengthening laboratory capacity, disease-surveillance and contact-tracing, case-management, risk-communications, case-management, disease-surveillance, the prevention and control of infections, and water, sanitation and hygiene; $5 million in ESF for cash assistance to vulnerable families adversely affected by COVID-19; and more than $1.3 million in MRA humanitarian assistance to support vulnerable people. The United States has invested more than $1.6 billion in total assistance for Sudan over the last 20 years, of which more than $3 million was for health.
- Tanzania: $3.4 million for health assistance funds the strengthening of laboratory capacity for optimal diagnostics, risk-communications, water and sanitation, the prevention and control of infections, public health messaging, and more. The United States has invested more than $7.5 billion total in Tanzania over the past 20 years, nearly $4.9 billion for health.
- Uganda: $3.6 million in assistance includes $2.3 million in health assistance to address the outbreak and nearly $1.3 million in MRA humanitarian assistance will support refugees and host communities in Uganda during the pandemic. The health assistance will strengthen the prevention and control of infections and case-management practices in health facilities, including by training health workers in new protocols; promote risk-communications and community engagement, including materials and messages to address most vulnerable groups; and improve management systems to ensure the accountability and availability of, and access to, health commodities, essential medicines, and health supplies in health facilities to maintain the continuity of services. This assistance is provided in addition to the nearly $8 billion in total U.S. Government investments for Uganda over the last 20 years and nearly $4.8 billion for health.
- Zambia: $3.4 million for health assistance will fund risk-communications, water and sanitation, the prevention and control of infections, public health messaging, and more. This new assistance joins $4.9 billion total U.S. Government investments for Zambia over the past 20 years, nearly $3.9 billion in U.S. health assistance.
- Zimbabwe: Nearly $5 million, including nearly $3 million for health assistance and $2 million for IDA humanitarian assistance will help to prepare laboratories for large-scale testing, support case-finding activities for influenza-like illnesses, implement a public-health emergency plan for points of entry, and more. The health assistance will fund the strengthening of laboratory capacity, the prevention and control and management of cases of COVID-19 in health facilities, including hand-washing stations, screening centers, preparing hospitals to be ready to treat COVID-19 patients, training health workers, and setting up alternative care-delivery points. Funding also will also support the training rapid-response teams, community health workers and volunteers; and risk communication and community engagement. This new assistance builds on a history of U.S. investments in Zimbabwe – nearly $3 billion total over the past 20 years, nearly $1.2 billion of which was for health.
- Regional Efforts in the Sahel: $5 million in ESF will strengthen the efforts of partner governments and civil society to manage and respond to COVID-19 with transparent communication and response. These investments will cover Burkina Faso, Niger, The Gambia, Chad, and Mali.
- Regional Efforts in West Africa: $5 million in ESF will go towards conducting information campaigns with local authorities and communities and engaging community groups, community radio stations, and local media actors to develop targeted messaging in local languages. This assistance will also engage citizens in local-led advocacy, dialogue, and inclusive behavior change. These investments will cover Cameroon, Côte d’Ivoire, Togo, Bénin, and Guinea.
- Regional Sub-Saharan Africa Humanitarian Assistance: More than $6 million in MRA humanitarian assistance to help vulnerable people during the pandemic.
Asia:
- Afghanistan: More than $18.7 million in U.S. assistance specifically provided for Afghanistan’s COVID-19 response includes more than $5.6 million for health and IDA humanitarian assistance to support the detection and treatment of COVID-19 for IDPs, and nearly $3.1 million in MRA humanitarian assistance for Afghan returnees. In addition, the United States has redirected $10 million in existing resources to support the United Nations Emergency Response Plan for COVID-19 to conduct disease-surveillance, improve laboratories, manage cases of the disease, prevent and control infections in health facilities, engage with local communities, and provide technical assistance to the Government of Afghanistan.
- Bangladesh: More than $25.7 million in assistance includes $10.3 million for health and IDA humanitarian assistance to help with case-management, surveillance activities, infection prevention and control, risk communication, and water, sanitation, and hygiene programs, and more than $15.3 million in MRA humanitarian support for vulnerable people during the pandemic, including refugees and host communities. This builds upon nearly $4 billion in total U.S. assistance over the past 20 years, which includes more than $1 billion for health.
- Bhutan: $1 million in total assistance for COVID-19 response includes $500,000 in ESF to support micro, small and medium-sized enterprises to generate income for those affected by COVID-19. It also includes $500,000 in health assistance to strengthen diagnostic laboratory capabilities and clinical case-management, provide virtual training for health care providers and lab personnel, and design and produce risk-communications materials. This assistance builds upon more than $6.5 million in total U.S. Government investments over the past 20 years, including $847,000 for health.
- Burma: Nearly $13.5 million total, including approximately $6.5 million for health and $4.8 million in IDA humanitarian assistance for the prevention and control of infections in health facilities, case-management, laboratories, risk-communications and community engagement, as well as water and sanitation supplies, including assistance to IDP camps that are facing water shortages. This also includes nearly $2.2 million in MRA humanitarian assistance to support vulnerable people and host communities during the pandemic. This assistance comes on top of long-term U.S. Government investments in Burma that total more than $1.3 billion over the past 20 years, which includes more than $176 million for health.
- Cambodia: More than $11 million in total assistance for the response to COVID-19 includes $5 million in ESF for relief and job-skills training for vulnerable people, such as returning migrants, and expanded efforts to counter trafficking and protect children. It also includes more than $6 million in health assistance to help the Cambodian Government prepare laboratory systems, activate case-finding and event-based surveillance, communicate risk, support technical experts for response and preparedness, and more. The U.S. Government has invested more than $1.6 billion in total assistance over the past 20 years, which includes more than $730 million for health.
- India: Nearly $5.9 million in health assistance to help India slow the spread of COVID-19, provide care for the affected, disseminate essential public health messages to communities, strengthen case-finding and surveillance, and mobilize innovative financing mechanisms for emergency preparedness and response to the pandemic. This builds on a foundation of nearly $2.8 billion in total assistance to India over the last 20 years, which includes more than $1.4 billion for health.
- Indonesia: $11 million includes more than $9 million in health and IDA humanitarian assistance to help the Indonesian Government prepare laboratory systems, activate case-finding and event-based surveillance, support technical experts for response and preparedness, and more. It also includes nearly $1.5 million in MRA humanitarian assistance for refugees, vulnerable migrants, and their host communities. The U.S. Government has invested more than $5 billion in total assistance over the past 20 years, including more than $1 billion for health.
- Kazakhstan: More than $3.1 million for health assistance will help prepare laboratory systems, activate case-finding and event-based surveillance, support technical experts for response and preparedness, bolster risk communication, and more. This new assistance builds upon U.S. investments of more than more than $2 billion in total assistance over the last 20 years, including $86 million for health.
- Kyrgyz Republic: Approximately $900,000 for health assistance will help prepare laboratory systems, activate case-finding and event-based surveillance, support technical experts for response and preparedness, bolster risk communication, and more. The United States has invested nearly $1.2 billion in total assistance for Kyrgyzstan over the past 20 years, including more than $120 million for health.
- Laos: Nearly $4.5 million for health assistance is helping the government prepare laboratory systems, activate case-finding and event-based surveillance, support technical experts for response and preparedness, and more. This assistance builds upon U.S. Government investment in Laos over time, including more than $348 million over the past decade, of which nearly $92 million was health assistance.
- Malaysia: $1.2 million total includes $1 million in health assistance that will fund the prevention and control of infections in health facilities, community engagement, disease-surveillance and contact-tracing systems, bolster risk-communications, and more in response to COVID-19. It also includes $200,000 in MRA humanitarian assistance to support COVID-19 response efforts for refugees and asylum seekers in Malaysia. This assistance builds upon a foundation of decades of U.S. investment in Malaysia, totaling more than $288 million over the past 20 years, including more than $3.6 million for health.
- Maldives: $2 million in ESF will support the expansion of social-protection services led by local civil-society organizations (CSOs) and assist them to advocate effectively for COVID recovery policies. Funding will provide technical assistance to the government to develop effective economic, fiscal, monetary measures in response to the COVID-19 pandemic. U.S. investments in Maldives include more than $30 million in total assistance since 2004.
- Mongolia: Nearly $1.2 million for health assistance is helping the Mongolian Government prepare laboratory systems, activate case-finding and event-based surveillance, and support technical experts for response and preparedness, and more. The United States has invested more than $1 billion in total assistance for Mongolia over the past 20 years, including nearly $106 million for health.
- Nepal: $7.3 million in total assistance includes $2.5 million in ESF to support local governments and disaster-management committees to respond to the economic and social impacts of COVID-19, and will provide small grants to the private sector and CSOs to enable economic recovery, mitigate food insecurity, and address the needs of vulnerable populations. It also includes $4.8 million for health assistance that is helping the Nepalese Government to conduct community-level risk-communications, prepare laboratory systems, activate case-finding and surveillance, support technical experts for response and preparedness, and more. Over the past 20 years, U.S. Government investment in Nepal totals more than $2 billion, including more than $603 million for health.
- Pacific Islands: Nearly $12.2 million total in assistance includes $5 million in ESF to strengthen the capacity of CSOs to combat disinformation and hate speech and to protect the rights of vulnerable and marginalized groups. Small grants also will be available at the community and national levels to increase their resilience and ability to respond to the economic impacts of COVID-19. This total also includes $4.7 million for health assistance, which is helping governments prepare laboratory systems, activate case-finding and event-based surveillance, support technical experts for response and preparedness; and $2.5 million in IDA humanitarian assistance to support risk-communications, the prevention and control of infectious diseases in health facilities, logistics, coordination efforts, and more. Over the last 20 years, the United States has invested over $5.21 billion in assistance to the Pacific Islands. Over the last decade, the United States has invested more than $620 million for health for the Pacific Islands.
- Papua New Guinea (PNG): $3.55 million for health assistance is helping the Government of PNG prepare laboratory systems, activate case-finding and event-based surveillance, and support technical experts for response and preparedness, risk-communications, the prevention and control of infectious diseases in health facilities, and more. The United States has invested over $108 million total in Papua New Guinea over the past 20 years, including more than $52 million for health.
- Pakistan: Nearly $18 million in total new assistance for Pakistan’s response to COVID-19 includes a $5 million contribution by USAID to the agreement between the Department of International Development of the United Kingdom with the Government of Pakistan to support its emergency cash-assistance program. USAID’s contribution will support about 66,000 vulnerable families affected by COVID-19; $10 million in health assistance to strengthen monitoring and better prepare communities to identify potential outbreaks, including funding for the training of healthcare providers and other urgent needs; and nearly $2.9 million in MRA humanitarian assistance to help vulnerable people in Pakistan. U.S. long-term investment in Pakistan over the past 20 years includes more than $18.4 billion in total assistance, which includes nearly $1.2 billion for health alone.
- The Philippines: More than $15 million in total COVID-19 assistance includes $5 million in ESF to provide grants and skills training to heavily affected sectors and communities; facilitate access to credit for micro and small enterprises; and support the efforts of the national government to improve crisis-management and procurement and promote a regulatory environment that enhances the resilience of communities and businesses;. In addition, about $6.5 million in health assistance and $2.8 million in IDA humanitarian assistance will help upgrade laboratories and specimen-transport systems, intensify case-finding and event-based surveillance; improve community-level preparedness and response; and support Filipino and international technical experts in risk-communications, the prevention and control of infectious diseases in health facilities, the promotion of handwashing and hygiene, and more. Finally, $875,000 in MRA humanitarian assistance will support vulnerable people during the pandemic. The United States has invested more than $4.5 billion in total assistance over the past 20 years, which includes $582 million in the Philippines’ health assistance.
- Sri Lanka: More than $5.8 million in total assistance includes $2 million in ESF to increase social services for areas and populations most affected by the COVID-19 crisis, address the specific threats to social cohesion, and mitigate negative economic impacts; $2 million in additional ESF for strengthening small and medium-sized enterprises and increasing women’s economic participation; and $1.3 million in health assistance to help the Sri Lankan Government prepare laboratory systems, activate case-finding and event-based surveillance, support technical experts for response and preparedness, conduct risk-communications, prevent and control infectious diseases in health facilities, and more. Finally, $590,000 in MRA humanitarian assistance will support vulnerable people during the pandemic. Over the past 20 years, U.S. assistance in Sri Lanka has totaled more than $1 billion, which includes $26 million for health.
- Tajikistan: Approximately $866,000 for health assistance is helping prepare laboratory systems, activate case-finding and event-based surveillance, support technical experts for response and preparedness, bolster risk-communications, and more. This support builds on more than $1 billion in total U.S. assistance over the past 20 years, which includes nearly $125 million for health.
- Thailand: More than $6.5 million for health assistance will help the Thai Government prepare laboratory systems, activate case-finding and event-based surveillance, support technical experts for response and preparedness, promote risk-communications, prevent and control infectious diseases in health facilities, and more. $730,000 in MRA humanitarian assistance will support surveillance and response capacity in all nine camps on the Thailand-Burma border hosting refugees from Burma. This new assistance builds upon long-term U.S. Government investments in Thailand of more than $1 billion in total assistance over the past 20 years, which includes nearly $214 million for health.
- Timor-Leste: Almost $1.1 million for health assistance is helping the Government of Timor-Leste prepare laboratory systems, activate case-finding and event-based surveillance, support technical experts for response and preparedness, bolster risk-communications, and more. The United States has invested more than $542 million in total assistance for Timor-Leste since independence in 2002, including nearly $70 million for health.
- Turkmenistan: Approximately $920,000 for health support has been made available to help prepare laboratory systems, activate case-finding and event-based surveillance, support technical experts for response and preparedness, bolster risk communication, and more. Over the past 20 years, the United States has collaborated closely with the Government of Turkmenistan and local partners to implement bilateral and regional programs totaling more than $207 million, including over $21 million in the health sector.
- Uzbekistan: Approximately $3.9 million in health funding is helping prepare laboratory systems, activate case-finding and event-based surveillance, support technical experts for response and preparedness, bolster risk-communications, and more. This COVID-19 response assistance builds on more than $1 billion in total assistance over the past 20 years, including more than $122 million in the health sector alone.
- Vietnam: Nearly $9.5 million in total assistance for response to COVID-19 includes $5 million in ESF, which will bring much-needed resources to bear immediately, including to support private-sector recovery by enhancing access to finance for businesses; improve firms’ capacity during an expected surge in demand; and working with the Government of Vietnam to bolster its relief interventions. It also includes $4.5 million in health assistance to help the Government prepare laboratory systems, activate case-finding and event-based surveillance, support technical experts for preparedness and response, conduct community education and engagement, prevent infections in health-care settings, public health screening at points of entry, and more. Over the past 20 years, the United States has invested more than $1.8 billion in total assistance for Vietnam, including more than $706 million for health.
- Regional Efforts in Asia: $2 million in ESF will provide essential services to vulnerable migrants in Central Asia stranded across the region as a result of border closures and ensure their safe return home in accordance with their own wishes and the help of NGOs and national governments. Additionally, $800,000 in health assistance is helping governments and NGOs across the region prepare laboratory systems, activate case-finding and event-based surveillance, support technical experts for response and preparedness, promote risk-communications, prevent and control infectious diseases in health facilities, and more. Furthermore, nearly $2.8 million in MRA humanitarian assistance will support vulnerable people in Southeast Asia and $425,000 in MRA humanitarian assistance will help vulnerable people in Central Asia during the pandemic. In addition to historic bilateral support to individual countries in the region, the United States has provided more than $226 million for health assistance regionally, and in total more than $3 billion in development and other assistance provided regionally over the last 20 years.
Europe and Eurasia:
- Albania: More than $2 million for health assistance is helping prepare laboratory systems, activate case-finding and event-based surveillance, support technical experts for response and preparedness, bolster risk-communications, and more. Over the last 20 years, the United States has invested more than $693 million in total assistance to Albania, including more than $51.8 million for health.
- Armenia: $2.7 million for health assistance is helping prepare laboratory systems, activate case-finding and event-based surveillance, support technical experts for response and preparedness, bolster risk-communications, and more. The United States has invested more than $1.57 billion in total assistance to Armenia over the past 20 years, including nearly $106 million for health.
- Azerbaijan: Nearly $3.6 million in total assistance includes $3 million in health assistance which is helping prepare laboratory systems, activate case-finding and event-based surveillance, support technical experts for response and preparedness, bolster risk-communications, and more. It also includes $565,000 in MRA humanitarian assistance that will help vulnerable people and host communities during the pandemic. Over the past 20 years, the United States has invested more than $894 million in total assistance to Azerbaijan, including nearly $41 million for health.
- Belarus: $1.7 million for health funding is helping prepare laboratory systems, activate case-finding and event-based surveillance, support technical experts for response and preparedness, bolster risk-communications, and more. This new assistance comes on top of decades of U.S. investment in Belarus, totaling more than $301 million over the past 20 years, including nearly $1.5 million for health.
- Bosnia and Herzegovina: $2.2 million for health assistance is helping prepare laboratory systems, activate case-finding and event-based surveillance, support technical experts for response and preparedness, bolster risk-communications, and more. The United States has invested more than $1.1 billion in total assistance for Bosnia and Herzegovina over the past 20 years, including $200,000 for health.
- Bulgaria: $500,000 in health assistance to address the outbreak. This new assistance builds on longstanding U.S. assistance for Bulgaria, which totals more than $558 million in total assistance over the past 20 years, including more than $6 million for health.
- Georgia: $2.7 million for health funding is helping prepare laboratory systems, activate case-finding and event-based surveillance, support technical experts for response and preparedness, bolster risk communication, and more. The United States has provided more than $3.6 billion in total U.S. assistance over the past 20 years, including nearly $139 million for health.
- Greece: Nearly $2.9 million in MRA humanitarian assistance will support COVID-19 response efforts for migrants and refugees in Greece. This new assistance builds upon a foundation of U.S. support for Greece, which totals more than $202 million in total investments over the last 20 years, including nearly $1.8 million for health.
- Italy: U.S. support includes $50 million in economic assistance implemented by USAID to bolster Italy’s response to COVID-19. USAID is expanding and supplementing the work of international organizations, non-governmental organizations, and faith-based groups responding to the pandemic in Italy and mitigating its community impact. USAID is also working with the Italian government to purchase health commodities and working to support Italian companies affected by the COVID-19 pandemic.
- Kosovo: Nearly $1.6 million in health assistance is helping prepare laboratory systems, activate case-finding and event-based surveillance, support technical experts for response and preparedness, bolster risk communication, and more. This assistance to combat COVID-19 is in addition to long-term U.S. investments, which total over $772 million in total assistance in Kosovo over the past 20 years, including more than $10 million for health.
- Moldova: Nearly $2.2 million for health assistance is helping prepare laboratory systems, activate case-finding and event-based surveillance, support technical experts for response and preparedness, bolster risk communication, and more. This COVID-19 assistance builds upon U.S. investments of more than $1 billion in total assistance over the past 20 years, including nearly $42 million for health.
- Montenegro: $300,000 in health assistance to address the outbreak. This new assistance joins long-term U.S. investment in Montenegro totaling more than $332 million, including more than $1 million for health.
- North Macedonia: $1.5 million for health assistance is helping prepare laboratory systems, activate case-finding and event-based surveillance, support technical experts for response and preparedness, bolster risk communication, and more. Over the past 20 years, the United States has invested more than $738 million in total assistance for North Macedonia, including nearly $11.5 million for health.
- Romania: $800,000 in health assistance to address the outbreak. In addition, the U.S. Government fully funded an operation by the North American Treaty Organization (NATO) to transport personal protective equipment (PPE) from South Korea to Romania. The United States has invested in Romania for decades, totaling nearly $700 million in total U.S. assistance in the last 20 years, including more than $55 million for health.
- Serbia: More than $2 million for health assistance is helping: expand testing, activate case-finding and event-based surveillance; deploy additional technical expertise for response and preparedness; bolster risk communication and community engagement; and improve hygiene practices in the home. The United States has invested more than $1 billion in total assistance to Serbia over the past 20 years, including nearly $5.4 million for health.
- Turkey: Nearly $5.7 million in MRA humanitarian assistance will support COVID-19 response efforts for refugees and host communities in Turkey. This new funding is in addition to the $18 million for Syrian refugee assistance inside Turkey announced March 3, and builds upon nearly $1.4 billion in total U.S. assistance to Turkey over the past 20 years, including more than $3 million for health assistance, helping lay the foundation for the current response.
- Ukraine: $15.5 million in total assistance includes $13.1 million in health and IDA humanitarian assistance that will improve the ability of local health care institutions to care for the sick and combat further spread of COVID-19 while increasing public communication to lower contagion risk. These funds will also mitigate secondary impacts such as loss of livelihoods and public services to vulnerable populations, including conflict-affected communities in eastern Ukraine. It also includes $2.4 million in MRA humanitarian assistance to support vulnerable populations during the pandemic. The United States has invested nearly $5 billion in total assistance to Ukraine over the past 20 years, including nearly $362 million for health.
- Regional Efforts in Europe and Eurasia: $5 million in ESF will empower civil society actors to safeguard democratic institutions and ensure citizens are heard during the pandemic. Funding will also assist civil society organizations to provide citizen oversight over their governments’ efforts to respond to COVID-19.
Latin America and the Caribbean:
- Argentina: $300,000 in new MRA humanitarian assistance will support COVID-19 response efforts for refugees and host communities. This funding is in addition to U.S. funding for Argentina over the past 20 years, $95.1 million total including nearly $696,000 for health.
- Bahamas: $750,000 in health assistance will increase risk communication and community engagement, infection prevention and control, surveillance and rapid response, and strengthen case management. This assistance comes in addition to decades of U.S. investment in the Bahamas, including nearly $143.1 million in total assistance over the past 20 years, $264,800 of which was for health.
- Belize: $300,000 in previously announced health assistance to address the outbreak and improve operational capacity and case-management. This assistance builds upon past U.S. investment in Belize, which totals more than $120 million over the past 20 years, including nearly $12 million for health.
- Bolivia: Nearly $900,000, including $750,000 in previously announced health assistance to build capacity in COVID-19 diagnostics and improve epidemiological surveillance; and $130,000 in new MRA humanitarian assistance will support COVID-19 response efforts for refugees and host communities. This assistance joins long-term U.S. investment in Bolivia, including nearly $2 billion in total U.S. assistance over the past 20 years, which includes $200 million for health.
- Brazil: Nearly $3.5 million, including $2 million in new health funding that will provide immediate support to vulnerable communities of the Amazon including risk communication and community engagement, infection prevention and control, water and sanitation activities, and surveillance and rapid response; $500,000 in new MRA humanitarian assistance to support COVID-19 response efforts for refugees and host communities; and $950,000 in previously announced ESF to incentivize private sector investments in mitigating non-health COVID impacts on rural and vulnerable urban populations. This assistance builds upon past U.S. investment in Brazil, which totals more than $617 million over the past 20 years, including nearly $103 million for health.
- Chile: $20,000 in new MRA humanitarian assistance to support COVID-19 response efforts for refugees and host communities. U.S. assistance to Chile totals $105.9 million over the 20 past years, including $914,000 for health.
- Colombia: Nearly $13.2 million in assistance for Colombia’s response to COVID-19 includes $8.5 million in previously announced IDA humanitarian assistance that is helping surveil the spread of the virus, provide water and sanitation supplies, manage COVID-19 cases, and more; and nearly $4.7 million in new and previously announced MRA humanitarian assistance, which will support efforts to help vulnerable people during the pandemic, including refugees, internally displaced persons, and host communities. In Colombia, the United States has invested nearly $12 billion in total assistance over the past 20 years, which includes approximately $32.5 million in health assistance.
- Costa Rica: Nearly $900,000 in total response to COVID-19 funding includes $800,000 in new health assistance and $80,000 in new MRA humanitarian assistance to support COVID-19 response efforts for refugees, vulnerable migrants, and host communities. U.S. funding in support of Costa Rica over the past 20 years totals $207 million, including $19.2 million in health assistance.
- Dominican Republic: Nearly $3.7 million in total response to COVID-19 funding includes $275,000 in MRA humanitarian assistance to support the COVID-19 response for refugees, vulnerable migrants, and host communities. This funding is in addition to $1.4 million in previously announced health assistance to address the outbreak, which is supporting epidemiological analysis and forecasting, contact-tracing, as well as pandemic surveillance; and $2 million in new ESF to address critical needs in the areas of social protection, psychosocial support, education, water and sanitation, and food security in vulnerable communities. . The United States has invested in the Dominican Republic’s long-term health and development through more than $1 billion in total U.S. assistance over the past 20 years, which includes nearly $298 million for health.
- Ecuador: More than $8.5 million in total response to COVID-19 funding includes $540,000 in new MRA humanitarian assistance to support the COVID-19 response effort for refugees and host communities. This assistance is in addition to the previously announced $2 million for health assistance that will increase testing capacity, implement risk communications and infection prevention activities, and strengthen clinical management; and $6 million in IDA humanitarian assistance that will provide support to transportation and logistics, as well as risk communication and community outreach efforts. Over the last 20 years, the United States’ long-term commitment to Ecuador includes more than $1 billion in total assistance, of which nearly $36 million for health assistance – helping Ecuador respond to other major public health challenges such as Zika and Malaria.
- El Salvador: Nearly $4.6 million in total response to COVID-19 funding includes $2 million in previously announced ESF to address second-order COVID-related impacts in El Salvador through job creation and increased access to credit, both critical factors in driving illegal immigration to the United States, and nearly $2.6 million for health assistance to address the outbreak. Support will include infection prevention, control, and case-management. Over the past 20 years, the United States has invested in El Salvador’s health and long-term development through more than $2.6 billion in total assistance, which includes $111 million for health.
- Guatemala: More than $2.4 million in previously announced health assistance for Guatemala will strengthen the health institutions to respond to COVID-19 in the areas of infection prevention and control, surveillance, risk communication, and clinical case-management. U.S. long-term investment in Guatemala’s health and development includes more than $2.6 billion in total U.S. assistance over the past 20 years, which includes $564 million for health.
- Guyana: $350,000 in new MRA humanitarian assistance to support the COVID-19 response effort for refugees and host communities. This assistance comes in addition to the regional COVID-19 response efforts in the Caribbean. Regionally, US assistance totaled $840 million total over the past 20 years, which includes $236 million for health.
- Haiti: $13.2 million in previously announced health and IDA humanitarian assistance for Haiti will support risk communication efforts, improve water and sanitation, prevent infections in health facilities, manage COVID-19 cases, strengthen laboratories, and more. The United States has invested nearly $6.7 billion in total assistance, including more than $1.8 billion for health in Haiti over the past 20 years.
- Honduras: More than $2.4 million for health assistance for Honduras will help the Government respond to the epidemic through focused support in the areas of lab strengthening, improved disease surveillance, and clinical management of COVID-19 cases. Some of these funds will also target infection control in migrant-receiving communities. The United States has also invested nearly $1.9 billion in total assistance, which includes $178 million for health, for Honduras over the past 20 years.
- Jamaica: $1 million in total health funding includes $300,000 in new funds supporting coordination, infection prevention, control, and management, risk communication efforts, and surveillance. This assistance builds upon U.S. investments of nearly $619 million total over the past 20 years, including nearly $87 million for health.
- Mexico: More than $1.8 million in MRA humanitarian funding will support COVID-19 response efforts for refugees, asylum seekers, vulnerable migrants, and host communities in Mexico. U.S. long-term investment in Mexico has helped build the foundation for Mexico’s COVID-19 response – this adds up to nearly $4.8 billion in total U.S. assistance over the past 20 years, including more than $61 million for health.
- Nicaragua: $750,000 in health assistance will provide training on infection prevention and control, pandemic management, and support for targeted communication and community engagement activities and community case management for the most at-risk populations for COVID-19.
- Panama: $825,000 in total response, including $750,000 in previously announced health assistance to optimize health system capacity to care for COVID-19 patients; and $75,000 in MRA humanitarian assistance to support the COVID-19 response for refugees, vulnerable migrants, and host communities. The United States has a history of investing in Panama’s health and long-term development with more than $425 million in total U.S. assistance over the past 20 years, including more than $33.5 million for health.
- Paraguay: Nearly $1.4 million in total response, including $1.3 million in previously announced health assistance to support risk communication efforts, infection control and prevention, clinical case-management, laboratory capacity strengthening, and surveillance; and $95,000 in MRA humanitarian assistance to support the COVID-19 response for refugees and host communities. U.S. investment in Paraguay is long-term and totals more than $456 million total over the past 20 years, including more than $42 million for health.
- Peru: Nearly $6 million in total response to COVID-19 funding includes $415,000 in new MRA humanitarian assistance to support the COVID-19 response for refugees and host communities; $3 million in previously announced ESF for addressing the economic impacts of COVID-19 and preventing backsliding on shared, top-level development and security issues, including the fight against the drug trade; and $2.5 million in previously announced health assistance to provide technical assistance and training in surveillance, infection prevention and control, risk communication, and community engagement. The United States’ strong history of investing in Peru’s health and long-term development has laid the foundation for Peru’s response, with more than $3.5 billion in total U.S. assistance over the last 20 years, including nearly $265 million for health.
- Trinidad and Tobago: $250,000 in new MRA humanitarian assistance to support the COVID-19 response for refugees and host communities. This assistance comes in addition to the regional COVID-19 efforts in the Caribbean, and historic assistance. Regionally, U.S. assistance totaled $840 million total over the past 20 years, which includes $236 million for health.
- Uruguay: $600,000 in total response to COVID-19 funding includes $500,000 in new health assistance for facilitating risk communication and community engagement, providing hygiene and medical supplies for health care facilities, and mitigating the secondary effects of the outbreak by continuing access to social-protection programs, and $100,000 in new MRA humanitarian assistance to support the COVID-19 response for migrants, refugees, and host communities. This assistance comes in addition to the more than $22 million in U.S. assistance provided to Uruguay over the past 20 years.
- Venezuela: More than $12.3 million previously announced total humanitarian assistance to the Venezuelan people is helping surveil the spread of the virus, provide water and sanitation supplies, manage COVID-19 cases, and more. In Venezuela, the U.S. has invested more than $278 million in total long-term assistance over the past 20 years, including more than $1.3 million in direct health assistance. In the last year, the U.S. provided additional lifesaving humanitarian assistance and development programming inside Venezuela that are not captured in COVID-19 response amounts.
- Regional Efforts in Central America: Nearly $850,000 in previously announced MRA humanitarian assistance will support regional efforts to respond to the Central America migration crisis to help vulnerable people in El Salvador, Guatemala, and Honduras during the pandemic.
- Regional Efforts in the Caribbean: $2.2 million in total health funding, including $500,000 in new funding to help 10 Caribbean countries (Antigua & Barbuda, Barbados, Dominica, Grenada, Guyana, St. Kitts and Nevis, Saint Lucia, St. Vincent and the Grenadines, Suriname, Trinidad and Tobago) scale up their risk communication efforts, provide water and sanitation, prevent and control infectious diseases in health facilities, manage COVID-19 cases, build laboratory capacity, and conduct surveillance. This builds upon decades of strategic U.S. investment in the region, including more than $840 million total over the past 20 years, which includes $236 million for health.
Middle East and North Africa:
- Algeria: $2 million in health assistance to support Algeria’s response to COVID-19 and mitigate its impact on Algerian society by strengthening risk communication and community engagement approaches under the Government of Algeria Preparedness and Response Plan.
- Iraq: More than $44 million in COVID-19 assistance for Iraq includes more than $33.1 million for health and IDA humanitarian assistance that is helping prepare laboratories, implement a public-health emergency plan for points of entry, activate case-finding and event-based surveillance for influenza-like illnesses, and more. The funding includes more than $10.8 million in MRA humanitarian assistance to assist vulnerable people during the pandemic, including refugees and host communities. This new assistance builds upon long-term investment in Iraq, which adds up to more than $70 billion in total U.S. assistance in the past 20 years, including nearly $4 billion in the health sector alone.
- Jordan: More than $8.4 million in assistance includes more than $6.9 million in MRA humanitarian assistance to support response to COVID-19 efforts to help vulnerable people in Jordan, including refugees and host communities, and $1.5 million in health assistance, which will support infection prevention and control to stop the spread of the disease, as well as laboratory strengthening for large-scale testing of COVID-19. The United States also is spearheading donor support to the Government of Jordan, coordinating life-saving assistance and prioritizing investments to respond rapidly now and to plan ahead as the threat evolves. Our investments in the last 20 years alone total more than $18.9 billion in total assistance, including more than $1.8 billion for health.
- Lebanon: $13.3 million in assistance for Lebanon includes $5.3 million in IDA humanitarian assistance for response to COVID-19 activities targeting vulnerable Lebanese, such as supporting private health facilities to properly triage, manage, and refer patients; ensure continuity of essential health services; carry out risk communication and community outreach activities, and increase access to water, sanitation, and hygiene. $8 million in MRA humanitarian assistance will support COVID-19 response efforts to help refugees and host communities in Lebanon. This assistance builds upon the nearly $4.9 billion in bilateral assistance, including more than $187 million for health assistance, that the U.S. has provided for Lebanon in the last 20 years. In addition to the bilateral funding, the U.S. has provided more than $2.3 billion in humanitarian assistance to respond to the Syria crisis in Lebanon.
- Libya: $12.4 million in response to COVID-19 includes $3.5 million in ESF to help municipalities to formalize their crisis response functions, develop emergency management plans, and train teams in Crisis Emergency Response. In addition, assistance will expand key public awareness, education, and guidance messages during the COVID-19 crisis. It also includes $6 million in IDA humanitarian assistance being provided for Libya to support risk communication, improve case-management, bolster coordination for an effective COVID-19 response, and strengthen infection prevention and control; and nearly $3 million in MRA humanitarian assistance to help vulnerable people during the pandemic, including refugees, vulnerable migrants, and host communities.
- Morocco: Nearly $7.7 million in total response to COVID-19 funding includes $4 million in ESF to support socio-economic recovery among marginalized and vulnerable populations in urban and rural populations through a cash relief program; and $3.7 million for health assistance that is helping prepare laboratory systems, activate case-finding and event-based surveillance, support technical experts for response and preparedness, bolster risk communication, and more. This assistance builds upon long-term U.S. investments in Morocco adding up to more than $2.6 billion in total assistance over the last 20 years, including $64.5 million for health.
- Syria: More than $31 million in humanitarian assistance for the response to COVID-19 in Syria supports risk communication, disease surveillance, water, sanitation and hygiene programs, infection prevention and control. This assistance joins decades of U.S. investments for the Syrian people, including more than $10 billion in humanitarian assistance for people in need inside Syria, Syrian refugees, and host communities since the beginning of the conflict. A number of U.S. sanctions exemptions and authorizations apply with respect to the provision of humanitarian assistance, including medicines and medical supplies, throughout Syria.
- Tunisia: $600,000 for health assistance will help prepare laboratory systems, activate case-finding and event-based surveillance, support technical experts for response and preparedness, bolster risk communication, and more. The United States has invested more than $1.3 billion in total U.S. assistance for Tunisia over the past 20 years, including more than $7 million for health.
- West Bank/Gaza: $5 million in IDA humanitarian assistance is helping provide immediate, life-saving assistance in the West Bank.
- Yemen: More than $2.5 million in humanitarian assistance will support COVID-19 response efforts to help refugees, vulnerable migrants, internally displaced persons, and host communities. In the past 20 years, the United States has provided nearly $4 billion in total assistance for Yemen’s long-term development, including nearly $132 million for health.
- Regional Efforts in the Middle East: $3 million in MRA humanitarian assistance to help vulnerable people during the pandemic.
Global:
- Approximately $92.1 million in global and regional health and humanitarian programming is being provided worldwide through international organizations and NGOs, including for programs that support supply-chain management, new partnerships, monitoring and evaluation, and more.
- $23 million to procure ventilators for key partners and Allies around the globe, fulfilling President Trump’s generous promises.
- Nearly $9.8 million in MRA humanitarian assistance for the global response to COVID-19 to address the challenges posed by the pandemic in refugee, vulnerable migrant, internally displaced persons, and host communities.
- $5 million in ESF for USAID’s Bureau for Democracy, Conflict, and Humanitarian Assistance (DCHA) will support civil society organizations (CSOs) to promote citizen-centered governance; respect for press and civic freedoms by monitoring legal protections for journalists and CSOs; provide legal assistance where COVID-related emergency laws have been used to restrict rights; ensure public health responses are non-discriminatory and counter efforts to blame or stigmatize marginalized groups related to COVID-19; promote media integrity and communicating responsible information on COVID-19; counter misinformation and disinformation; ensure the financial sustainability of independent media outlets. and provide support to human rights defenders to carry out their important work.
- Nearly $4.3 million in ESF for USAID’s Bureau for Economic Growth, Education, and Environment (E3) to expand trade and access to education. With approximately $750,000 USAID will provide technical assistance and surge capacity to partner governments and USAID Missions on education responses to COVID-19, create a Global Working Group on Distance Learning in Crisis, and launch a Virtual Center of Excellence for Education Distance Learning for developing countries. With $3.5 million USAID will support a global public-private partnership to support partner governments to reduce trade barriers on medical devices and testing kits/instruments, and improve governments’ adherence to international standards for medical equipment.
- $8 million in ESF for USAID’s Bureau for Resilience and Food Security (RFS) will support a multi-partner effort to mitigate pandemic-related shocks to the global food and agriculture system. Some policy responses in emerging economies to the pandemic are already negatively impacting local food systems, and food insecurity, hunger and malnutrition are growing concerns. USAID will produce data and analysis to help countries implement forward-looking policies; help small and medium-sized food and agriculture businesses shift business models and withstand the most severe impacts; and rapidly disseminate information in emerging economies about how consumers can safely participate in food and agriculture activities and markets amid COVID-19. The partnership includes collaborating with finance sector partners to unlock financing for small and medium-sized food and agribusinesses.
- $2 million in ESF is planned for the Secretary of State’s Office of Global Women’s Issues (S/GWI) to ensure survivors of gender-based violence (have access to emergency assistance, improved protections, and justice. The funds also intend to support advocacy and awareness campaigns on the gendered economic, governance, and security implications of GBV, particularly as it relates to the COVID-19 pandemic.
- The United States is the largest and most reliable contributor to dozens of international organizations, including UNICEF and the UN Office for the Coordination of Humanitarian Affairs. These contributions include significant investments in core operating budgets, which sustain the organizational structure and support functions that enable global humanitarian, development, peacebuilding, and other actions, and ensure consistent oversight for, and the effectiveness and efficiency of, U.S. government assistance in countries around the world.
FULL DOCUMENT: https://www.state.gov/update-the-united-states-continues-to-lead-the-global-response-to-covid-19/
_________________
ORGANISMS
CORONAVIRUS
IMF. 05/19/2020. TRACKING THE $9 TRILLION GLOBAL FISCAL SUPPORT TO FIGHT COVID-19
- Bryn Battersby, Senior Economist in the Public Financial Management division of the Fiscal Affairs Department.
- W. Raphael Lam, Senior Economist in the Fiscal Affairs Department.
- Elif Ture, Economist in the Fiscal Affairs Department.
Governments have put forward swift and significant emergency lifelines to protect people in response to the pandemic. We measured these in the April 2020 Fiscal Monitor and as countries have stepped up their efforts, we have updated the numbers.
So, where does the global fiscal support stand now?
The total is about $9 trillion, or $1 trillion more than the estimates just over a month ago. The breakdown looks like this: direct budget support is currently estimated at $4.4 trillion globally, and additional public sector loans and equity injections, guarantees, and other quasi-fiscal operations (such as non-commercial activity of public corporations) amount to another $4.6 trillion.

Onward and upward
The upward revision was largely because of a second wave of measures by governments as the economic fallout from the pandemic proves more severe.
For example, the United States approved an additional fiscal package of $483 billion on April 23. Japan revised its initially conditional cash transfers program into a universal one to provide an additional $83 billion in support to households on April 20, while France and Korea introduced additional measures such as transfers to support households.
As in April, the Group of Twenty (G20) advanced and emerging market economies account for the bulk of the global fiscal support—$8 trillion. The total revenue and spending measures for G20 countries account for 4.5 percent of GDP on average, larger than those during the global financial crisis.
The fiscal measures take various forms and have different budgetary and debt-related implications.
The estimates focus on discretionary revenue and spending measures but exclude deferral of taxes and social security contributions to the extent possible. We exclude them because they involve a temporary delay of revenue, which would be collected in the future (sometimes within the same fiscal year). The estimates also include separate classification for governments’ provision of loans and equity injection that have an immediate effect on the government balance sheet, as well as guarantees that expose the governments to risks if the guarantees were called in down the road.
The IMF will continue providing timely updates of countries’ fiscal support in response to the COVID-19 pandemic. You can find more country specific measures from the Fiscal Monitor here (PDF). You can find out more about countries’ broader policies, including fiscal, monetary and financial policies to fight the pandemic in the IMF policy tracker.
Paul Elger, Susan Yang, and Yuan Xiang worked on the Fiscal Monitor and have contributed to this blog.
FULL DOCUMENT: https://blogs.imf.org/2020/05/20/tracking-the-9-trillion-global-fiscal-support-to-fight-covid-19/?utm_medium=email&utm_source=govdelivery
WTO. 20/05/2020. WTO TRADE BAROMETERS. WTO goods barometer flashes red as COVID-19 disrupts world trade
The volume of world merchandise trade is likely to fall precipitously in the first half of 2020 as the COVID-19 pandemic disrupts the global economy, according to the WTO Goods Trade Barometer released on 20 May. The index currently stands at 87.6, far below the baseline value of 100, suggesting a sharp contraction in world trade extending into the second quarter. This is the lowest value on record since the indicator was launched in July 2016.
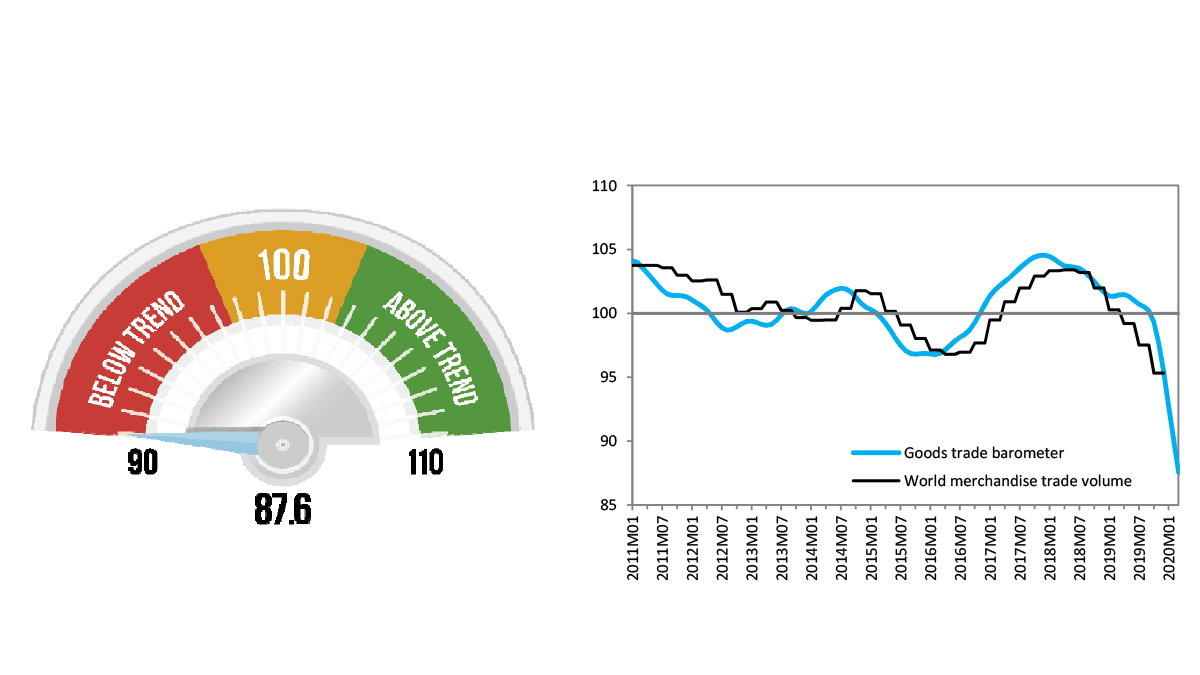
The Goods Trade Barometer provides real-time information on the trajectory of world merchandise trade relative to recent trends. The current reading captures the initial phases of the COVID-19 outbreak, and shows no sign of the trade decline bottoming out yet. This measure is consistent with the WTO's trade forecast issued on 8 April 2020, which estimated that world merchandise trade could decline by between 13% and 32% in 2020, depending on the duration of the pandemic and the effectiveness of policy responses.
All of the barometer's component indices are currently well below trend. The automotive products index (79.7) was weakest of all, due to collapsing car production and sales in major economies. The sharp decline in the forward-looking export orders index (83.3) suggests that trade weakness will persist in the short-run. Declines in the container shipping (88.5) and air freight (88.0) indices reflect weak demand for traded goods as well as supply-side constraints arising from efforts to suppress COVID-19. Only the indices for electronic components (94.0) and agricultural raw materials (95.7) show signs of stability, although they too remain below trend.
Trade had already been slowing in 2019 before the pandemic, weighed down by persistent trade tensions and weakening economic growth. WTO trade statistics show that the volume of world merchandise trade shrank by 0.1% in 2019, marking the first annual decline since 2009, during the global financial crisis. Trade was relatively weak in the final quarter of 2019, but this is unlikely to have been influenced by COVID-19, which was first detected very late in the year.
Like its counterpart for services, the Goods Trade Barometer aims to gauge momentum and identify turning points in global trade growth. As such, it complements trade statistics and forecasts from the WTO and other organizations. Readings of 100 indicate growth in line with medium-term trends; readings greater than 100 suggest above-trend growth, while those below 100 indicate below-trend growth.
FULL DOCUMENT: https://www.wto.org/english/news_e/news20_e/wtoi_19may20_e.htm
INTERNATIONAL TRADE
WTO. 20/05/2020. WTO TRADE BAROMETERS. WTO goods barometer flashes red as COVID-19 disrupts world trade
The volume of world merchandise trade is likely to fall precipitously in the first half of 2020 as the COVID-19 pandemic disrupts the global economy, according to the WTO Goods Trade Barometer released on 20 May. The index currently stands at 87.6, far below the baseline value of 100, suggesting a sharp contraction in world trade extending into the second quarter. This is the lowest value on record since the indicator was launched in July 2016.
The Goods Trade Barometer provides real-time information on the trajectory of world merchandise trade relative to recent trends. The current reading captures the initial phases of the COVID-19 outbreak, and shows no sign of the trade decline bottoming out yet. This measure is consistent with the WTO's trade forecast issued on 8 April 2020, which estimated that world merchandise trade could decline by between 13% and 32% in 2020, depending on the duration of the pandemic and the effectiveness of policy responses.
All of the barometer's component indices are currently well below trend. The automotive products index (79.7) was weakest of all, due to collapsing car production and sales in major economies. The sharp decline in the forward-looking export orders index (83.3) suggests that trade weakness will persist in the short-run. Declines in the container shipping (88.5) and air freight (88.0) indices reflect weak demand for traded goods as well as supply-side constraints arising from efforts to suppress COVID-19. Only the indices for electronic components (94.0) and agricultural raw materials (95.7) show signs of stability, although they too remain below trend.
Trade had already been slowing in 2019 before the pandemic, weighed down by persistent trade tensions and weakening economic growth. WTO trade statistics show that the volume of world merchandise trade shrank by 0.1% in 2019, marking the first annual decline since 2009, during the global financial crisis. Trade was relatively weak in the final quarter of 2019, but this is unlikely to have been influenced by COVID-19, which was first detected very late in the year.
Like its counterpart for services, the Goods Trade Barometer aims to gauge momentum and identify turning points in global trade growth. As such, it complements trade statistics and forecasts from the WTO and other organizations. Readings of 100 indicate growth in line with medium-term trends; readings greater than 100 suggest above-trend growth, while those below 100 indicate below-trend growth.
FULL DOCUMENT: https://www.wto.org/english/news_e/news20_e/wtoi_19may20_e.htm
________________
ECONOMIA BRASILEIRA / BRAZIL ECONOMICS
CORONAVÍRUS
FGV. IBRE. 19/05/20. Coronavírus
A intenção do Ministério da Economia de vincular a prorrogação ou permanência do auxílio emergencial a uma revisão de outros gastos sociais como o abono salarial, o farmácia popular e o seguro-defeso, conforme divulgado nesta terça-feira (19) na mídia, apesar de atacar políticas consideradas ineficientes, não é uma solução simples para financiar esse programa, avalia Manoel Pires, pesquisador associado do FGV IBRE.
“Apesar de ser uma medida racional, pois pode melhorar a distribuição de renda focando a população mais vulnerável, é politicamente difícil”, analisa, lembrando que programas assistenciais como o abono salarial demandam emenda constitucional para serem alterados. “Iniciativas semelhantes já foram tentadas e rejeitadas. Na reforma da Previdência aprovada no ano passado já se propôs a redução do abono, mas isso não passou”, ressalta.
Para o pesquisador, equacionar a extensão de um programa de auxílio à renda com o desafio fiscal pós-crise sanitária demandará, invariavelmente, uma mudança na estrutura de tributação, para torna-la mais progressiva. “Evidente que uma ampliação do auxílio depende do que se consegue economizar, mas também envolve o que se está disposto a propor de redistribuição de renda. E aí já não estaremos falando de ganhos incrementais, mas de algo de potencial transformador”, afirma. Para isso, entretanto, será preciso rediscutir a reforma tributária em outras bases, já que a proposta que avançava no Congresso, lembra Pires, não tratava de tributação direta. “Além disso, considero mais difícil retomá-la nesse momento em que o setor de serviços – que mais seria impactado com a mudança proposta – já está perdendo muito com os efeitos da pandemia”, afirma.
Pires lembra que o auxílio emergencial de R$ 600 representará um gasto de 2% do PIB nos três meses de duração atualmente prevista, e subiria para 8% se anualizado. “Se for comparado com a ajuda recebida por um beneficiário típico do Bolsa Família, é um valor alto. Se excluirmos esses beneficiários da conta, entretanto, falamos de um cenário de rendimento muito disperso, em que a renda do informal média gira em torno de R$ 1,7 mil, e para estes o benefício é baixo”, compara. Uma primeira tarefa na eventual extensão do programa, afirma, é a redução de brechas para evitar fraudes. “Para isso, por exemplo, seria preciso ampliar a segurança jurídica no cruzamento de bases de dados para refinar a seleção de beneficiários, para evitar que regras sejam derrubadas na justiça”, afirma, citando o exemplo da determinação judicial de cessão do benefício a pessoas com irregularidades no CPF.
Em encontro virtual de pesquisadores do IBRE com jornalistas do Valor Econômico do qual participou, Pires já havia destacado que a pressão política para a extensão do benefício é grande, especialmente com o prolongamento da fase aguda do contágio pelo coronavírus e a possibilidade de lockdown nas regiões mais afetadas, como São Paulo. Desse encontro ainda participaram o pesquisador Fernando Veloso, o diretor do IBRE Luiz Guilherme Schymura, e Vinícius Botelho, ex-secretário de Avaliação e Gestão da Informação do Ministério da Cidadania e ex-pesquisador do IBRE. Em matéria que reúne o conteúdo dessa conferência virtual (o conteúdo pode estar restrito a assinantes), publicada nesta segunda-feira (18/5), os economistas reforçaram a necessidade de se discutir as distorções presentes no modelo atual do auxílio. Na Conjuntura Econômica de maio, o diretor do Centro de Políticas Sociais da FGV Marcelo Neri também havia defendido a necessidade de filtrar essa política, “para que se consiga manter a ajuda por mais tempo, a quem mais precisa”.
DOCUMENTO: https://portalibre.fgv.br/navegacao-superior/noticias/coronavirus-13.htm
INFLAÇÃO
FGV. IBRE. 20/05/20. Índices Gerais de Preços. IGP-M Segundo Decêndio. IGP-M varia 0,01% na 2ª prévia de maio
O Índice Geral de Preços - Mercado (IGP-M) variou 0,01% no segundo decêndio de maio. No segundo decêndio de abril, este índice apresentou taxa de 1,00%.
“A queda de braço entre os preços dos alimentos e dos combustíveis segue influenciando o resultado do IGP. Em maio, as fontes de pressão se inverteram no IPA. A taxa do grupo alimentação desacelerou e os preços dos combustíveis passaram a cair menos. Os aumentos autorizados nas refinarias devem contribuir para aceleração do IGP-M até o final do mês”, afirma André Braz, Coordenador dos índices de Preços.
O Índice de Preços ao Produtor Amplo (IPA) passou de 1,36% no segundo decêndio de abril para 0,18% no segundo decêndio de maio. Na análise por estágios de processamento, os preços dos Bens Finais intensificaram a queda passando de -0,02% em abril para -0,33% em maio. A maior contribuição para este resultado partiu do subgrupo alimentos in natura, cuja taxa passou de 8,18% para -0,90%.
O índice referente a Bens Intermediários variou -1,39% no segundo decêndio de maio, ante 0,23% no mesmo período de abril. O destaque coube ao subgrupo materiais e componentes para a manufatura, cuja taxa passou de 3,21% para 0,08%.
A taxa do grupo Matérias-Primas Brutas foi de 3,93% no segundo decêndio de abril para 2,26% em igual período de maio. Contribuíram para o movimento do grupo os seguintes itens: bovinos (-3,07% para 0,35%), aves (-4,39% para -2,12%) e cana-de-açúcar (0,76% para 1,72%). Em sentido oposto, destacam-se os itens milho (em grão) (3,00% para -7,62%), soja (em grão) (8,26% para 4,44%) e café (em grão) (9,44% para 0,77%).
O Índice de Preços ao Consumidor (IPC) caiu 0,59% no segundo decêndio de maio, após alta de 0,28% no mesmo período de coleta de abril. Todas as classes de despesa componentes do índice registraram decréscimo em suas taxas de variação, com destaque para o grupo Transportes (-1,04% para -2,74%). Nesta classe de despesa, vale mencionar o comportamento do item gasolina, cuja taxa passou de -3,59% para -8,93%.
Também foram computados decréscimos nas taxas de variação dos grupos Educação, Leitura e Recreação (0,41% para -1,77%), Alimentação (1,42% para 0,45%), Habitação (0,38% para -0,09%), Saúde e Cuidados Pessoais (0,46% para 0,24%), Vestuário (-0,08% para -0,27%), Despesas Diversas (0,41% para 0,31%) e Comunicação (0,06% para 0,02%). Nestas classes de despesa, os maiores recuos foram observados nas taxas dos itens: passagem aérea (6,82% para -15,08%), hortaliças e legumes (8,99% para 3,80%), tarifa de eletricidade residencial (0,47% para -0,58%), artigos de higiene e cuidado pessoal (0,85% para 0,22%), roupas (0,00% para -0,19%) e alimentos para animais domésticos (2,30% para 0,44%) e tarifa de telefone residencial (0,36% para 0,03%).
O Índice Nacional de Custo da Construção (INCC) variou 0,21% no segundo decêndio de maio. No mês anterior, o índice foi de 0,22%. Os três grupos componentes do INCC apresentaram as seguintes variações na passagem do segundo decêndio de abril para o segundo decêndio de maio: Materiais e Equipamentos (0,57% para 0,58%), Serviços (0,15% para -0,03%) e Mão de Obra que não variou pelo segundo mês consecutivo.
DOCUMENTO: https://portalibre.fgv.br/navegacao-superior/noticias/igp-m-varia-0-01-na-2-previa-de-maio.htm
CNI. 20/05/2020. Queda da atividade industrial registra novo recorde negativo entre março e abril. Mais da metade da capacidade instalada das empresas ficou ociosa. Redução do nível de produção e número de empregados são os mais intensos e disseminados da série histórica

A Sondagem Industrial divulgada nesta quarta-feira (20), pela Confederação Nacional da Indústria (CNI), mostra um recuo sem precedentes na atividade industrial brasileira tanto em intensidade quanto em alcance, entre março e abril deste ano, devido aos efeitos da crise provocada pelo coronavírus. O índice de evolução da produção registrou 26 pontos em uma escala de 0 a 100. Nessa metodologia, os valores abaixo de 50 pontos mostram queda.
A nova contração da atividade industrial provocou o recuo de 9 pontos percentuais da utilização da capacidade instalada entre março e abril, para 49%. Esse dado mostra que mais da metade da capacidade instalada da indústria ficou ociosa em abril. E a forte queda no número de empregados levou o índice para 38,2 pontos em abril, bem distante da linha divisória de 50 pontos. Esse é o menor de toda a série mensal iniciada em 2011.
“A maior disseminação da crise entre as empresas no mês de abril era esperada, pois, no início do mês de março, grande parte da indústria ainda não tinha sentido a queda na demanda. Em abril, as empresas passaram todo o mês sob os efeitos das medidas de distanciamento social”, diz o gerente executivo de Pesquisa e Competitividade, Renato da Fonseca.
Apesar disso, os índices que medem as expectativas tiveram uma ligeira melhora. No entanto, mostram significativo pessimismo do empresário para os próximos seis meses, com queda de demanda, exportações, compras de matérias-primas e número de empregados. A intenção de investir segue baixa.
Sondagem Industrial. Queda da atividade industrial se intensifica em abril
Os impactos da crise causada pela pandemia da Covid-19 já haviam sido sentidos em março, após queda da demanda que forçou uma redução da atividade industrial. Em abril, os efeitos sobre a atividade se intensificaram e se disseminaram ainda mais entre as empresas, de forma que a atividade industrial registrou nova contração.

DOCUMENTO: https://bucket-gw-cni-static-cms-si.s3.amazonaws.com/media/filer_public/da/02/da022749-0b07-478a-859f-1e925ea1b483/sondagemindustrial_abril2020.pdf
OPEP. REUTES. 20 DE MAIO DE 2020. Produção de petróleo russa cai para perto de cota acertada com Opep+, dizem fontes
Por Olesya Astakhova
MOSCOU (Reuters) - A produção de petróleo e gás condensado da Rússia caiu para 9,42 milhões de barris por dia entre 1° de maio e 19 de maio, em meio a efeitos de um acordo global para redução de produção, disseram à Reuters duas fontes com conhecimento dos dados.
O pacto para restrição de oferta fechado entre a Organização dos Países Exportadores de Petróleo (Opep), a Rússia e outros produtores, um grupo conhecido como Opep+, entrou em vigor em 1° de maio.
O gás condensado, um tipo de petróleo leve não incluído no pacto da Opep, responde por entre 700 mil e 800 mil bpd da produção combinada de líquidos da Rússia, o que significa que a produção de petróleo foi de cerca de 8,72 milhões de bpd. Isso é próximo da cota acertada com a Opep+, de 8,5 milhões de bpd de petróleo.
A produção de petróleo e condensado da Rússia em abril foi de 11,35 milhões de bpd.
O ministério de Energia da Rússia não respondeu a um pedido de comentário.
INDÚSTRIA
CNI. 20/05/2020. Queda da atividade industrial registra novo recorde negativo entre março e abril. Mais da metade da capacidade instalada das empresas ficou ociosa. Redução do nível de produção e número de empregados são os mais intensos e disseminados da série histórica
A Sondagem Industrial divulgada nesta quarta-feira (20), pela Confederação Nacional da Indústria (CNI), mostra um recuo sem precedentes na atividade industrial brasileira tanto em intensidade quanto em alcance, entre março e abril deste ano, devido aos efeitos da crise provocada pelo coronavírus. O índice de evolução da produção registrou 26 pontos em uma escala de 0 a 100. Nessa metodologia, os valores abaixo de 50 pontos mostram queda.
A nova contração da atividade industrial provocou o recuo de 9 pontos percentuais da utilização da capacidade instalada entre março e abril, para 49%. Esse dado mostra que mais da metade da capacidade instalada da indústria ficou ociosa em abril. E a forte queda no número de empregados levou o índice para 38,2 pontos em abril, bem distante da linha divisória de 50 pontos. Esse é o menor de toda a série mensal iniciada em 2011.
“A maior disseminação da crise entre as empresas no mês de abril era esperada, pois, no início do mês de março, grande parte da indústria ainda não tinha sentido a queda na demanda. Em abril, as empresas passaram todo o mês sob os efeitos das medidas de distanciamento social”, diz o gerente executivo de Pesquisa e Competitividade, Renato da Fonseca.
Apesar disso, os índices que medem as expectativas tiveram uma ligeira melhora. No entanto, mostram significativo pessimismo do empresário para os próximos seis meses, com queda de demanda, exportações, compras de matérias-primas e número de empregados. A intenção de investir segue baixa.
Sondagem Industrial. Queda da atividade industrial se intensifica em abril
Os impactos da crise causada pela pandemia da Covid-19 já haviam sido sentidos em março, após queda da demanda que forçou uma redução da atividade industrial. Em abril, os efeitos sobre a atividade se intensificaram e se disseminaram ainda mais entre as empresas, de forma que a atividade industrial registrou nova contração.
DOCUMENTO: https://bucket-gw-cni-static-cms-si.s3.amazonaws.com/media/filer_public/da/02/da022749-0b07-478a-859f-1e925ea1b483/sondagemindustrial_abril2020.pdf
ENERGIA
OPEP. REUTES. 20 DE MAIO DE 2020. Produção de petróleo russa cai para perto de cota acertada com Opep+, dizem fontes
Por Olesya Astakhova
MOSCOU (Reuters) - A produção de petróleo e gás condensado da Rússia caiu para 9,42 milhões de barris por dia entre 1° de maio e 19 de maio, em meio a efeitos de um acordo global para redução de produção, disseram à Reuters duas fontes com conhecimento dos dados.
O pacto para restrição de oferta fechado entre a Organização dos Países Exportadores de Petróleo (Opep), a Rússia e outros produtores, um grupo conhecido como Opep+, entrou em vigor em 1° de maio.
O gás condensado, um tipo de petróleo leve não incluído no pacto da Opep, responde por entre 700 mil e 800 mil bpd da produção combinada de líquidos da Rússia, o que significa que a produção de petróleo foi de cerca de 8,72 milhões de bpd. Isso é próximo da cota acertada com a Opep+, de 8,5 milhões de bpd de petróleo.
A produção de petróleo e condensado da Rússia em abril foi de 11,35 milhões de bpd.
O ministério de Energia da Rússia não respondeu a um pedido de comentário.
________________
LGCJ.: